|
Leprosy
Leprosy is caused by M. leprae and predominantly affects the skin and peripheral nerves. The disease is endemic in many tropical and subtropical countries but is declining in prevalence as a result of multidrug therapy. The Indian subcontinent, Southeast Asia, sub-Saharan countries in Africa, and Brazil comprise the areas most affected at present . The mode of transmission of leprosy is unknown, but it is probably inhalation of bacilli, which may be excreted from the nasal passages of a multi bacillary patient or possibly implanted from organisms in the soil. Direct person-to-person infection by means of the skin occurs rarely if at all. After inhalation, it is likely that bacilli pass through the blood to peripheral and cutaneous nerves, where infection and host reaction commence.
|
|
Immunopathologic Spectrum of Leprosy
The sequence of disease pathogenesis is complex, is very chronic, and depends on host-parasite immunologic responses. The leprosy bacillus is nontoxic, and clinicopathologic manifestations are the result of immunopathology and/or the progressive accumulation of infected cells. Leprosy is the best example of a disease showing an immunopathologic spectrum whereby the host immune reaction to the infective agent ranges from apparently none to marked, with a consequent range of clinicopathologic manifestations . Tuberculoid leprosy indicates a high cellular immune response (l.e., T cells and macrophage activation) and few bacilli in tissues; at the opposite pole, lepromatous leprosy indicates an absent cellular immune response to M. leprae antigens, with no macrophage activation and abundant bacilli in tissues. The spectrum of leprosy is a continuum, and patients may move in either direction according to host response and treatment. The standard delineation follows that of Ridley and Jopling, with categories defined along the spectrum by a combination of clinical, microbiologic, histopathologic, and immunologic indices: TT (tuberculoid), BT (borderline tuberculoid), BB (midborderline), BL (borderline lepromatous), and LL (lepromatous). The term borderline is used to denote patterns that share some features of both tuberculoid and lepromatous leprosy .
TT and LL patients are stable, the former often self-healing and the latter remaining heavily infected unless given appropriate chemotherapy. Patients presenting at the BT point will often downgrade toward BL leprosy in the
|
|
absence of treatment. The central point of the spectrum (BB) is the most unstable, with most patients downgrading to LL if not treated. The term indeterminate leprosy is used to describe patients presenting with very early leprosy lesions that cannot be categorized definitely along the immunopathologic spectrum (e.g., cannot be determined as BT or LL).
|
|
It is likely that in endemic zones, a high proportion of people are infected by M. leprae but either have full immunity and no disease or have developed one or a few lesions that have self-healed without significant morbidity. Patients with determined leprosy are most numerous at the BT and LL points of the spectrum.
|
|
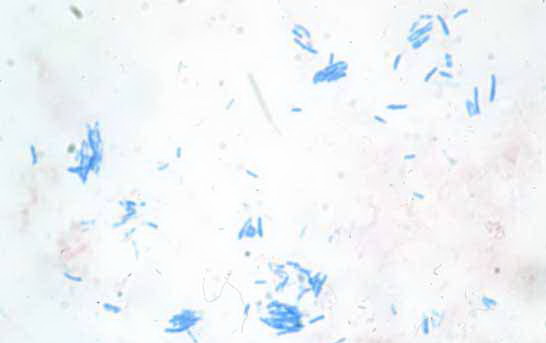
Staining of Mycobacterium leprae Bacilli
The classical method for demonstrating leprosy bacilli in lesions is a modified Ziehl-Neelsen stain, where the degree of acid and alcohol removal of carbol fuchsin is less than in the methods used for identifying other mycobacteria. The Fite methods are the most commonly used . Methanamine silver stains are also useful in detecting fragmented acid-fast bacilli. The sensitivity of detection of acid-fast bacilli by histologic means remains poor, because about 1,000 bacilli per cubic centimeter of tissue must be present in order to detect 1 bacillus in a section. For lesions where bacilli are scanty, it is recommended that at least six sections be examined before declaring them negative (144). The standard enumeration of leprosy bacilli in lesions-the bacterial index (BI)follows Ridley's logarithmic scale (which applies to both skin biopsies and slit skin smears).
|
BI = 0: no bacilli observed
|
- · BI = 1: 1 to 10 bacilli in 10 to 100 high-power fields (hpf, oil immersion)
- · BI = 2: 1 to 10 bacilli in 1 to 10 hpf
- · BI = 3: 1 to 10 bacilli per hpf
- · BI = 4: 10 to 100 bacilli per hpf
- · BI = 5: 100 to 1,000 bacilli per hpf
- · BI = 6: >1,000 bacilli per hpf
|
|
|
Solid-staining bacilli indicate that the organisms are capable of multiplication. Fragmented (beaded) and granular acid-fast
|
|
bacilli indicate that they are dead. Patients with no bacilli detectable in lesions are termed paucibacillary; those with some or many bacilli are multibacillary (this distinction is important in determing the duration of chemotherapy) .
|
|
Immunocytochemical methods for demonstrating mycobacterial antigens have a limited role. The most frequently used is a polyclonal anti-BeG antibody . In untreated lesions, it will not detect small numbers of bacilli if ordinary histochemical methods have proved negative. However, immunocytochemistry does have a role in demonstrating the presence of leprosy antigen after the bacilli have fragmented, been partly digested by macrophage enzymes, and lost their acid-fast staining quality .
|
|
Clinical Pathology of Leprosy
For general discussions of clinical leprosy and leprosy pathology, the reader is referred to Job (147) and Britton and Lockwood .
|
|
Early, Indeterminate Leprosy
Many patients present with obvious or advanced skin and peripheral nerve lesions (the latter are primarily nerve enlargement and the consequences of anesthesia). These patients have "determined leprosy." However, the earliest detectable skin lesion comprises one or a few hypopigmented macules with variable loss of sensation. Any part of the body may be affected.
|
|
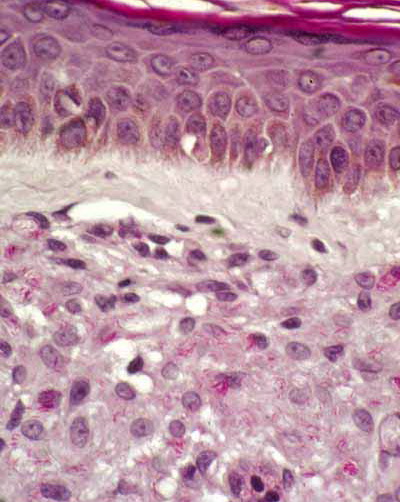
Histopathology.
There is mild lymphocytic and macrophage accumulation around neurovascular bundles, the
|
|
superficial and deep dermal vessels, sweat glands, and erector pili muscle; focal lymphocytic invasion into the lower epidermis and into the dermal nerves may be observed. No formed epithelioid cell granulomas are present (if they were, it would not be indeterminate leprosy but a tuberculoid leprosy). Schwann cell hyperplasia is a feature, but it is highly subjective. Not all of these features are present in every case. The diagnosis hinges on finding one or more acid-fast bacilli in the sites of predilection: in nerve, in erector pili muscle, just under the epidermis, or in a macrophage about a vessel. Without demonstrating bacilli, the diagnosis can only be presumptive .
|
|
A distinctive variant of lepromatous leprosy, the histoid type, first described in 1963 (149), is characterized by the occurrence of well-demarcated cutaneous and subcutaneous nodules resembling dermatofibromas. It frequently follows incomplete chemotherapy or acquired drug resistance, leading to bacterial relapse.
|
|
Rarely, lepromatous leprosy can present as a single lesion rather than as multiple lesions (150).
|
|
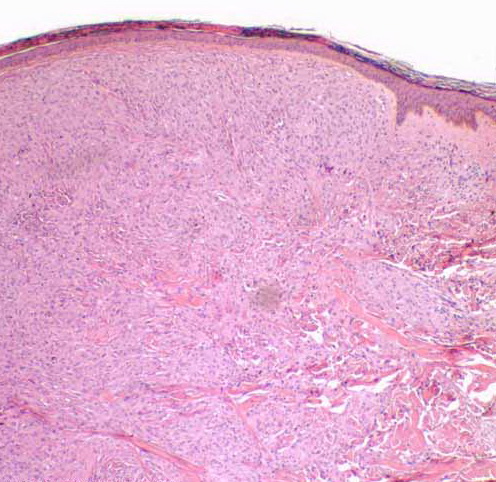
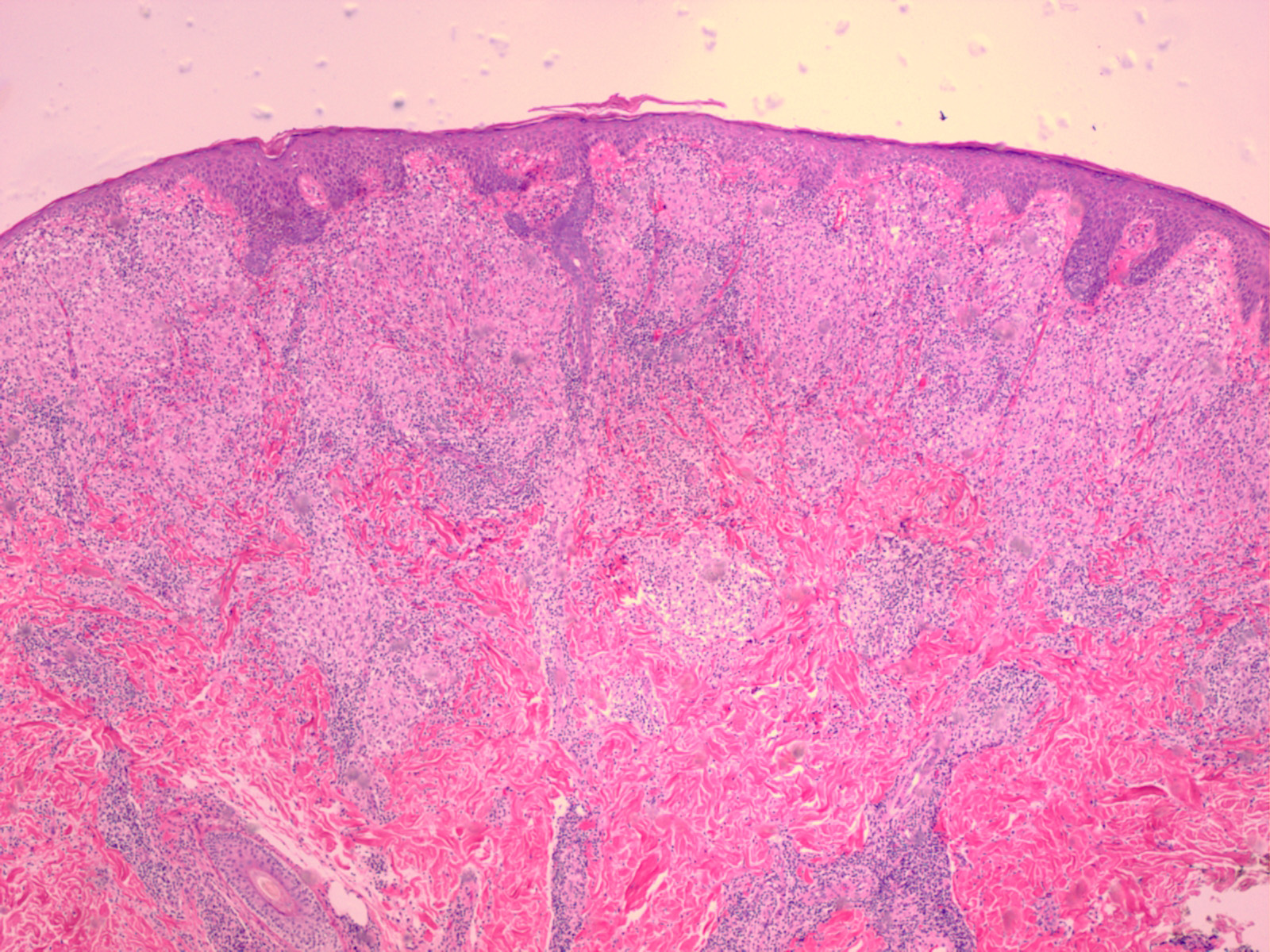
Histopathology.
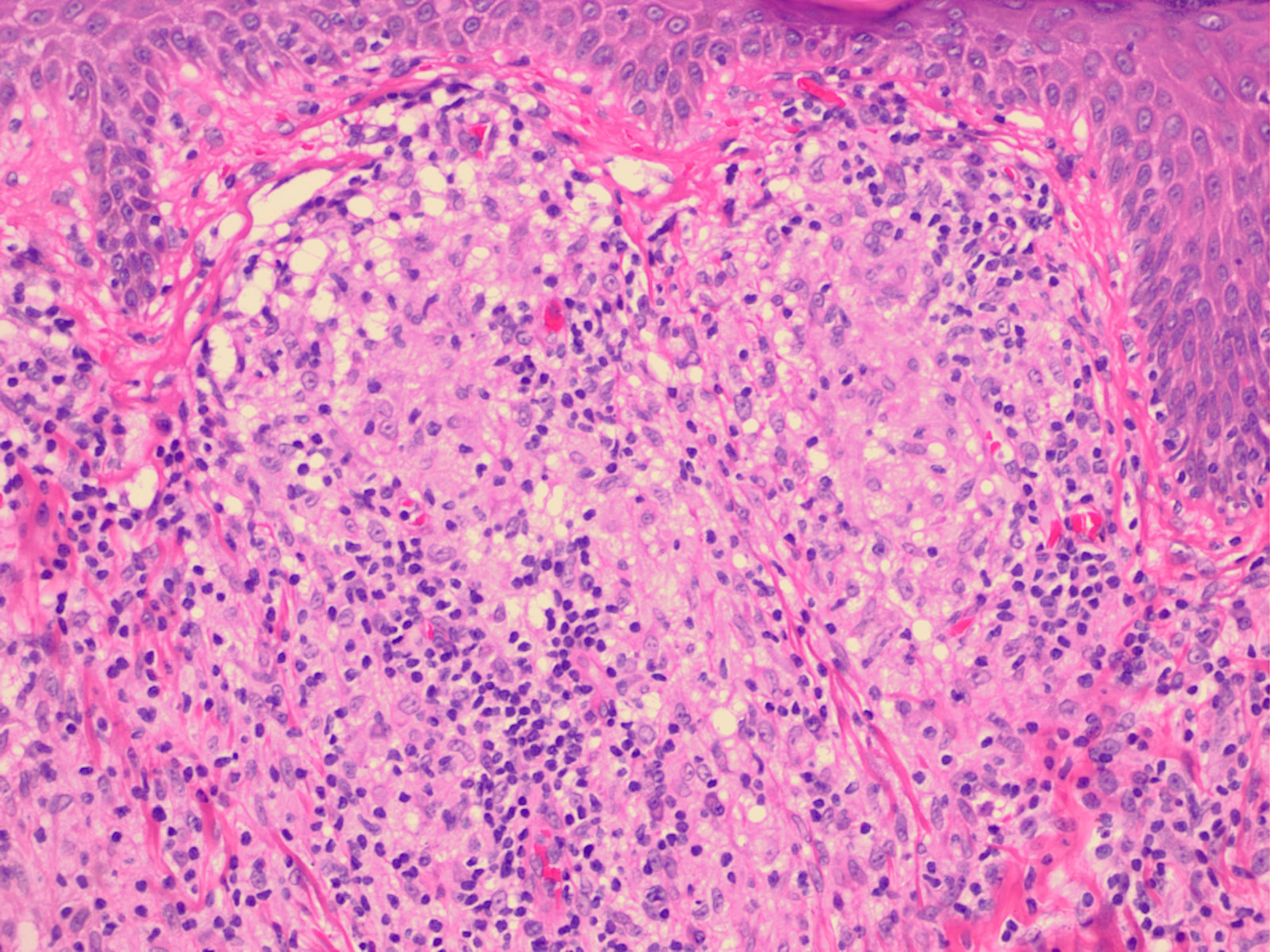
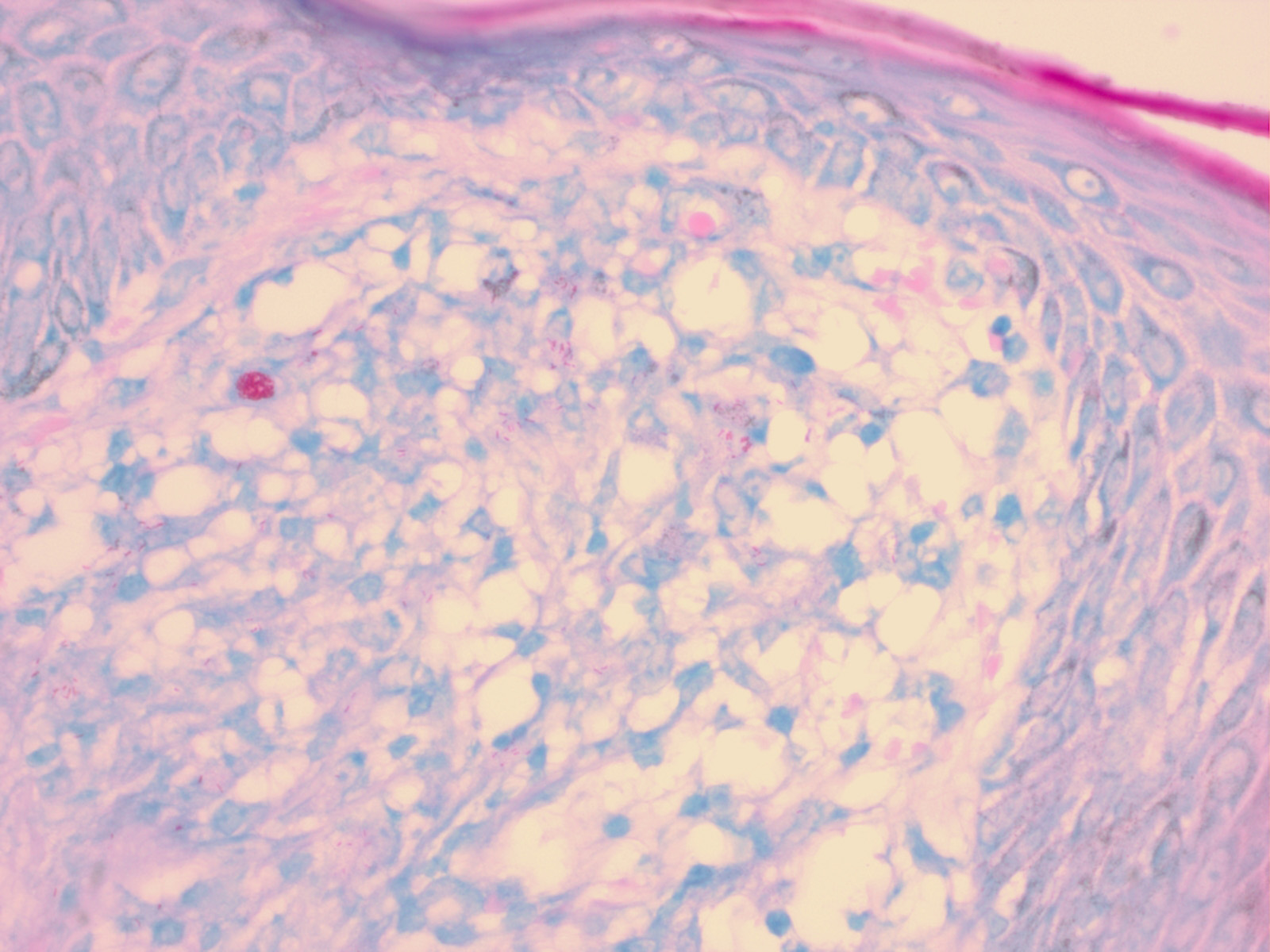
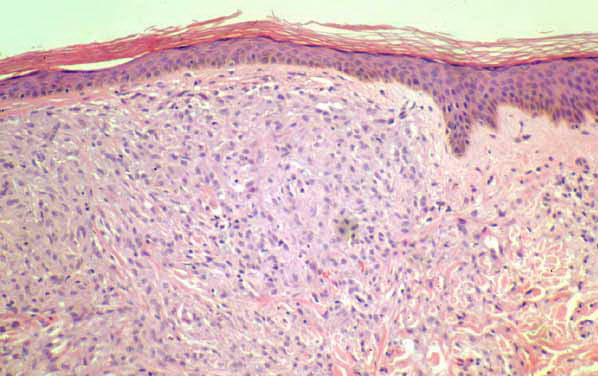
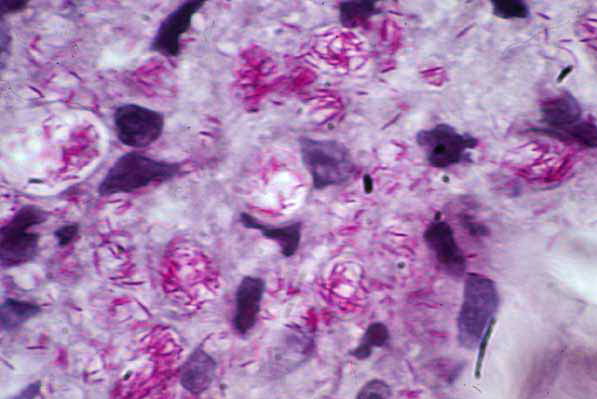
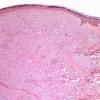
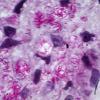
Lepromatous leprosy, in the usual macular or infiltrative-nodular lesions, exhibits an extensive cellular infiltrate that is almost invariably separated from the flattened epidermis by a narrow grenz zone of normal collagen (Figs. 21-35 and 21-36). The infiltrate causes the destruction of the cutaneous appendages and extends into the subcutaneous fat. In florid early lesions, the macrophages have abundant eosinophilic cytoplasm and contain a mixed population of solid and fragmented bacilli (Bl = 4 or 5) (Figs. 21-33). The bacilli, on Wade-Fite staining, can be seen to measure about 5.0 by 0.5 IJm and if solid may be packed like cigars. Bacilli are commonly observed in endothelial cells as well (Fig. 21-37). There is no macrophage activation to form epithelioid cell granulomas. Lymphocyte infiltration is not prominent, but there may be many plasma cells.
|
|
In time, and with anti mycobacterial chemotherapy, degenerate bacilli accumulate in the macrophages-the socalled lepra cells or Virchow cells-which then have foamy or vacuolated cytoplasm (Fig. 21-38). They resemble xanthoma cells and, on staining with fat stains, are shown to contain lipid-largely neutral fat and phospholipidsrather than cholesterol. The Wade-Fite stain reveals that the bacilli are fragmented or granular and, especially in very chronic lesions, disposed in large basophilic clumps called globi. In lepromatous leprosy, in contrast to tuberculoid leprosy, the nerves in the skin may contain considerable numbers of leprosy bacilli but remain well preserved for a long time and slowly become fibrotic.
|
|
Histoid Leprosy
Histoid leprosy shows the highest loads of bacilli (frequently, the Bl is 6), and the majority are solid staining, arranged in clumps like sheaves of wheat. The macrophage reaction is unusual in that the cells frequently become spindle shaped and oriented in a storiform pattern, similar to those of a fibrohistiocytoma . The epidermis may be stretched over such dermal expansile nodules.
|
|
Histopathology.
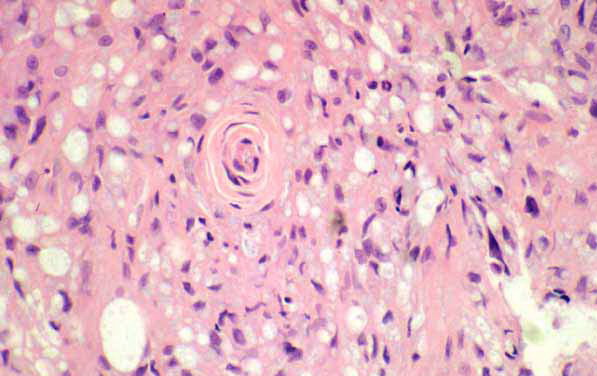
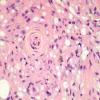
The important difference between LL and BL leprosy histology is that in BL, the lymphocytes are more prominent and there is a tendency for some activation of macrophages to form poorly to moderately defined granulomas. Perineural fibroblast proliferation, forming an "onion skin" in cross-section, is typical. Foamy cells are not prominent, and globi do not usually accumulate; the Bl ranges from 4 to 5.
|
|
Midborderline Leprosy
In midborderline (BB) leprosy, the skin lesions are irregularly dispersed and shaped erythematous plaques with punched-out centers. There may be small satellite lesions. Edema is prominent in the lesions.
|
|
Histopathology. In BB leprosy, the macro phages are uniformly activated to epithelioid cells but are not focalized into distinct granulomas, and lymphocytes are scanty. There are no Langhans giant cells. The Bl ranges from 3 to 4. Dermal edema is prominent between the inflammatory cells.
|
|
Borderline Tuberculoid Leprosy
In borderline tuberculoid (BT) leprosy, the lesions are asymmetrical and may be scanty. They are dry, hairless plaques with central hypopigmentation. Nerve enlargement is usually found, and the lesions are usually anesthetic.
|
|
Histopathology. Granulomas with peripheral lymphocytes follow the neurovascular bundles and infiltrate sweat glands and erector pili muscles. Langhans giant cells are variable in number
|
|
and are not large in size. Granulomas along the superficial vascular plexus are frequent, but they do not infiltrate up into the epidermis. Nerve erosion and obliteration are typical . Acid-fast bacilli are scanty (81 ranges from 0 to 2) and most readily found in the 8chwann cells of nerves. Immunocytochemical staining for 8-100 protein often demonstrates the perineural and intraneural granuloma well .
|
|
Tuberculoid Leprosy
The skin lesions of tuberculoid (TT) leprosy are scanty, dry, erythematous, hypopigmented papules or plaques with sharply defined edges. Anaesthesia is prominent (except on the face). The number of lesions ranges from one to five. Thickened local peripheral nerves may be found. The lesions heal rapidly on chemotherapy.
|
|
Histopathology
. Primary TT leprosy has large epithelioid cells arranged in compact granulomas along with neurovascular bundles, with dense peripheral lymphocyte accumulation. Langhans giant cells are typically absent. Dermal nerves may be absent (obliterated) or surrounded and eroded by dense lymphocyte cuffs. Acid-fast bacilli are rarely found, even in nerves. A second pattern of TT leprosy is found in certain reactional states (see next page).
|
|
Peripheral Nerves
In all of these patterns of leprosy, the major peripheral nerves are often undergoing parallel pathologies. The inflammation is similar, and the same classification system is applied. However, the density of acid-fast bacilli is often a logrithm higher than in the nearby skin (151).
|
|
Leprosy Reactions
Leprosy reactions are classified into two main types (1 and 2). A third reaction is specific to Lucio multibacillary leprosy
|
|
Type 1 Reactions
Because the immunopathologic spectrum of leprosy is a continuum, patients may move along it in both directions. Should such shifts be rapid, they induce an inflammatory reaction with edema that results in enlargement of lesions with more erythema . Shifts toward the tuberculoid pole are called upgrading or reversal reactions; shifts toward the lepromatous pole are termed downgrading reactions. Both are aspects of delayed hypersensitivity, or type 1, leprosy reactions. TT patients are stable. BT patients may downgrade without treatment. Multibacillary patients, particularly those at the BL point, frequently upgrade on chemotherapy, and about one quarter of them will exhibit significant reactions. BB patients are most unstable and will move either way depending on therapy, often with reactions. The most important aspect of type 1 reactions is not the skin but the condition of the peripheral nerves, in which a similar inflammatory process is going on; reaction induces increased intraneural inflammation and edema, which is damaging. At worst, there is caseous necrosis of large peripheral nerves resulting from upgrading reactions.
|
|
Histopathology. The histopathology of type 1 reactions has still not been well evaluated . The distinction between upgrading and downgrading reactions is difficult to make and may require serial examinations. Typically,
|
|
there is edema within and about the granulomas and proliferation of fibrocytes in the dermis. In upgrading reactions, the granuloma becomes more epithelioid and activated, and Langhans giant cells are larger ; there may be erosion of granulomas into the lower epidermis, and there may be fibrinoid necrosis within granulomas and even within dermal nerves. In downgrading reactions, necrosis is much less common, and over time the density of bacilli increases. Multibacillary leprosy patients who upgrade on therapy show old foamy macrophages and degenerate bacilli admixed with new epithelioid cell granulomas.
|
|
type 2 Reaction: Erythema Nodosum Leprosum
Erythema nodosum leprosum (ENL) occurs most commonly in LL leprosy and less frequently in BL leprosy. It may be observed not only in patients under treatment but also in untreated patients. Clinically, the reaction has a greater resemblance to erythema multiforme than to erythema nodosum.
|
|
On the skin, tender, red plaques and nodules together with areas of erythema, and occasionally also purpura and vesicles, are observed. Ulceration, however, is rare. The eruption is widespread and accompanied by fever, malaise, arthralgia, and leukocytosis. New lesions appear for only a few days in some cases but for weeks and even years in others. This is the only type of reactional leprosy that responds to treatment with thalidomide.
|
|
Histopathology. In ENL, the lesions are foci of acute inflammation superimposed on chronic multibacillary leprosy . Polymorph neutrophils may be scanty or so abundant as to form a dermal abscess with ulceration . Whereas foamy macrophages containing fragmented bacilli are usual, in some patients no bacilli remain and macrophages have a granular pink hue on Wade-Fite staining, indicating mycobacterial debris. An
anti mycobacterial immunocytochemical stain (e.g., anti-BCG) will indicate abundant antigen. A necrotizing vasculitis affecting arterioles, venules, and capillaries occurs in some cases of ENL; these patients may have superficial ulceration.
|
|
The Lucio reaction occurs exclusively in diffuse lepromatous leprosy, in which it is a fairly common complication. It
|
|
usually occurs in patients who have received either no treatment or inadequate treatment. In contrast to ENL, fever, tenderness, and leukocytosis are absent. The lesions consist of barely palpable, hemorrhagic, sharply marginated, irregular plaques. They develop into crusted lesions and, particularly on the legs, into ulcers. There may be repeated attacks or continuous appearance of new lesions for years.
|
|
Histopathology. In the Lucio reaction, vascular changes are critical . Endothelial proliferation leading to luminal obliteration is observed in association with thrombosis in the medium-sized vessels of the dermis and subcutis. There is a sparse, largely mononuclear infiltrate. Dense aggregates of acid-fast bacilli are found in the walls and the endothelium of normal-appearing vessels as well as in vessels with proliferative changes . Ischemic necrosis, brought on by the vascular occlusion, leads to hemorrhagic infarcts and results in crusted erosions or frank ulcers.
|
|
Electron Microscopy of Leprosy
Under electron microscopy, M. leprae can be seen to consist of an electron-dense cytoplasm lined by a trilaminal plasma membrane. Outside of this membrane lies the bacterial cell wall surrounded by a radiolucent area, the waxy coating typical of mycobacteria (81). Lepra bacilli are found in the skin, predominantly in macrophages and in Schwann cells.
|
|
Pathogenesis of Leprosy
With respect to immunologic reactivity, patients with lepromatous leprosy have a defect in cell-mediated immune responses to the lepra bacilli, which therefore cannot be eradicated from the body spontaneously . The primary defect lies in the T lymphocytes, which can be stimulated only slightly or not at all to react against the lepra bacilli and thus do not adequately activate macrophages to destroy phagocytosed bacilli. This defect is specific for M. leprae, because patients with lepromatous leprosy show normal immunologic responses to antigens other than lepromin in both in vivo and in vitro testing.
|
|
The specific inability of T lymphocytes obtained from patients with lepromatous leprosy to react against lepromin is shown by the fact that when these lymphocytes are incubated with lepromin, they show little or no production of macrophage migration-inhibiting factor (MIF). In contrast, the lymphocytes of patients with tuberculoid leprosy produce significant amounts of MIF on exposure to lepromin. One modem view is that in tuberculoid patients, exposure to leprosy antigens results in a predominant T helper 1 (Th-1) cytokine secretion profile, which results in macrophage activation. Conversely, in lepromatous patients, the cytokine profile (Th-2) inhibits cell-mediated immunity and promotes humoral immunity, which does not contribute to host defense . In reversal reactions, there is an increase in the lymphocyte response to lepromin during the reaction and a decrease during the postreaction phase.
Analysis of T-cell subsets in lesions has shown that in tuberculoid leprosy, with its high degree of resistance to the leprosy bacilli, the T helper lymphocytes are distributed evenly throughout the epithelioid cell aggregates, and the suppressor T lymphocytes are restricted to the peripheries of the granulomas. In lepromatous leprosy, both helper and suppressor T lymphocytes are distributed diffusely throughout the lesions . It is noteworthy that the distribution of helper and suppressor T cells in tuberculoid leprosy is similar to that observed in sarcoidosis.
|
|
In patients with either ENL or the Lucio reaction, deposits of IgG and the third component of complement (C3), as well as circulating immune complexes, have been found in the vessel walls of the dermal lesions. This suggests that both reactions are mediated by immune complexes (Gell and Coombes type III reaction) .
|
|
The lepromin skin test, or Mitsuda test, consists of the intradermal injection of a preparation of M. leprae derived from autoclaved infected human tissue. A positive reaction consists of the formation of a nodule measuring :<:5 mm in diameter after 2 to 4 weeks. On histologic examination, the nodule shows an epithelioid cell granuloma. The reaction is positive only in the high-resistance (tuberculoid and borderline tuberculoid) forms of the disease. In indeterminate leprosy, it may be positive or negative. The test reveals the inability of patients at the lepromatous end of the spectrum to react to the injection of M. leprae with an epithelioid cell granuloma, and its main value is therefore as a marker of specific cell-mediated immunity to this organism, which varies continuously along the immunopathologic spectrum.
|
|
HIV Infection and Leprosy
Because HIV induces a generalized immunosuppressive state, and because a wide range of intracellular infectious agents normally controlled by the T-cell/macrophage system may proliferate to cause significant disease, it was expected that leprosy might also be affected. Specifically, the disease might become more prevalent in HIVand leprosy coendemic areas, and individual patients might downgrade toward lepromatous disease as their HIV disease progresses. However, epidemiologic studies have shown no effect of HIV infection on the incidence of leprosy in properly controlled studies (159, 160) nor has a change in the proportions of tuberculoid versus lepromatous patients been noted (161). At present, the only clinicopathologic difference between HIV-infected and noninfected leprosy patients that is suggested is an increased likelihood of HIV-positive patients undergoing type 1 upgrading reactions . This rather paradoxical phenomenon awaits further evaluation.
|
|
Histopathologic Differential Diagnosis
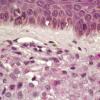
The leprosy bacillus cannot yet be grown in vitro. Tuberculoid (granulomatous) leprosy needs to be distinguished from the many other granulomatous dermatitides. The presence of acid-fast bacilli in nerves is conclusive proof of leprosy, as is the demonstration of an intraneural granuloma. The S-100 stain may highlight this phenomenon (163), although in practice, if the diagnosis is in doubt after investigation with ordinary stains, this immunocytochemical method is not usually diagnostic either. In leprosy, naked granulomas are found only in BB leprosy, and acid-fast bacilli will be found in the lesions. Sarcoidosis may rarely cause granulomas to form within peripheral nerves (164) but does not appear to do so in dermal nerves. The general vertical perineurovascular distribution of granulomatous inflammation and involvement of sweat glands in tuberculoid leprosy are helpful. The presence or absence of plasma cells or of intraepidermal lymphocytes is not helpful. Unlike other mycobacterial skin infections such as tuberculosis, and unlike granulomatous leishmaniasis, the epidermis in tuberculoid leprosy is usually flat and non hyperplastic. Late secondary and tertiary cutaneous syphilis is characterized by epithelioid and giant cell granulomas in the dermis, not directly involving nerves, and the epithelium is usually hyperplastic. Intragranuloma necrosis (fibrinoid or caseating) occurs in leprosy in type 1 reactions, sometimes spontaneously; this can be confused with necrobiotic lesions such as granuloma annulare. Necrosis within a nerve that is granulomatous is diagnostic of leprosy.
|
|
Early, indeterminate leprosy overlaps with many specific and nonspecific dermatitides manifesting perineurovascular lymphocytic infiltrates. Finding bacilli in critical sites (in nerve, under the epidermis, in erector pili muscle, or in macrophages) is critical. In the absence of bacilli and the presence of a pandermal infiltrate, leprosy can only be suspected. Problems may arise from contaminant mycobacteria in staining solutions and in the water baths used for floating out sections. Such organisms are usually above the plane of the section, overlap the cell nuclei, and usually stain darker than M. leprae. The use of PCR for identifying paucibacillary leprosy in skin sections and tissues has not been as successful as it once was thought to be
|
|
Ultimately, there is a proportion of suspect paucibacillary leprosy lesions for which the histopathologist cannot make a firm diagnosis either way, and intra- and interobserver variation may be considerable (166). Clinical diagnosis of single-lesion leprosy is also imperfect .
|
|
Lepromatous leprosy infiltrates can resemble xanthoma, although the cytoplasmic granularity is coarser in the latter disease. The presence of acid-fast bacilli is obviously important, and in long-treated lesions that may cause confusion, anti mycobacterial immunocytochemistry is helpful. ENL may be overlooked because it is a combined
|
|
chronic and acute inflammatory infiltrate, but once thought of, the presence of bacilli or antigen is diagnostic. Certain other mycobacterioses in immunosuppressed patients, such as M. avium-intracellulare, may produce histoid-like multibacillary lesions ; however, nerves are not involved in this infection.
|
|
|
|
|