|
Bullous lupus erythematosus = الذئبة الحمامية الفقاعية |
 |
 |
 |
|
Bullous Systemic Lupus Erythematosus
Vesicles and bullae may develop in patients with SLE. In contrast to dermatitis herpetiform is, the lesions are not symmetrical and do not have a predilection for extensor surfaces of arms, elbows, or scalp; they may be photodistributed or widespread and are not pruritic. These patients rarely have classic lesions of discoid, systemic, or subacute cutaneous lupus erythematosus when they develop blisters. In cases from the literature, the vast majority of patients have had a previous history of lupus erythematosus, and most authors have required definitive American Rheumatologic Association criteria before making the diagnosis in those patients with bullous lesions. Uncommonly, patients (who later developed other stigmata of lupus) have presented with a blistering eruption but without previous signs or symptoms of connective tissue disease. Bullous lupus erythematosus is most common in women, particularly black women. Most of these cases were exquisitely sensitive to dapsone therapy, with rapid involution of the lesions. No correlation with clinical activity of lupus erythematosus was apparent. Some patients with EBA will progress to SLE.
|
|
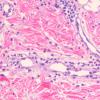
Histopathology.
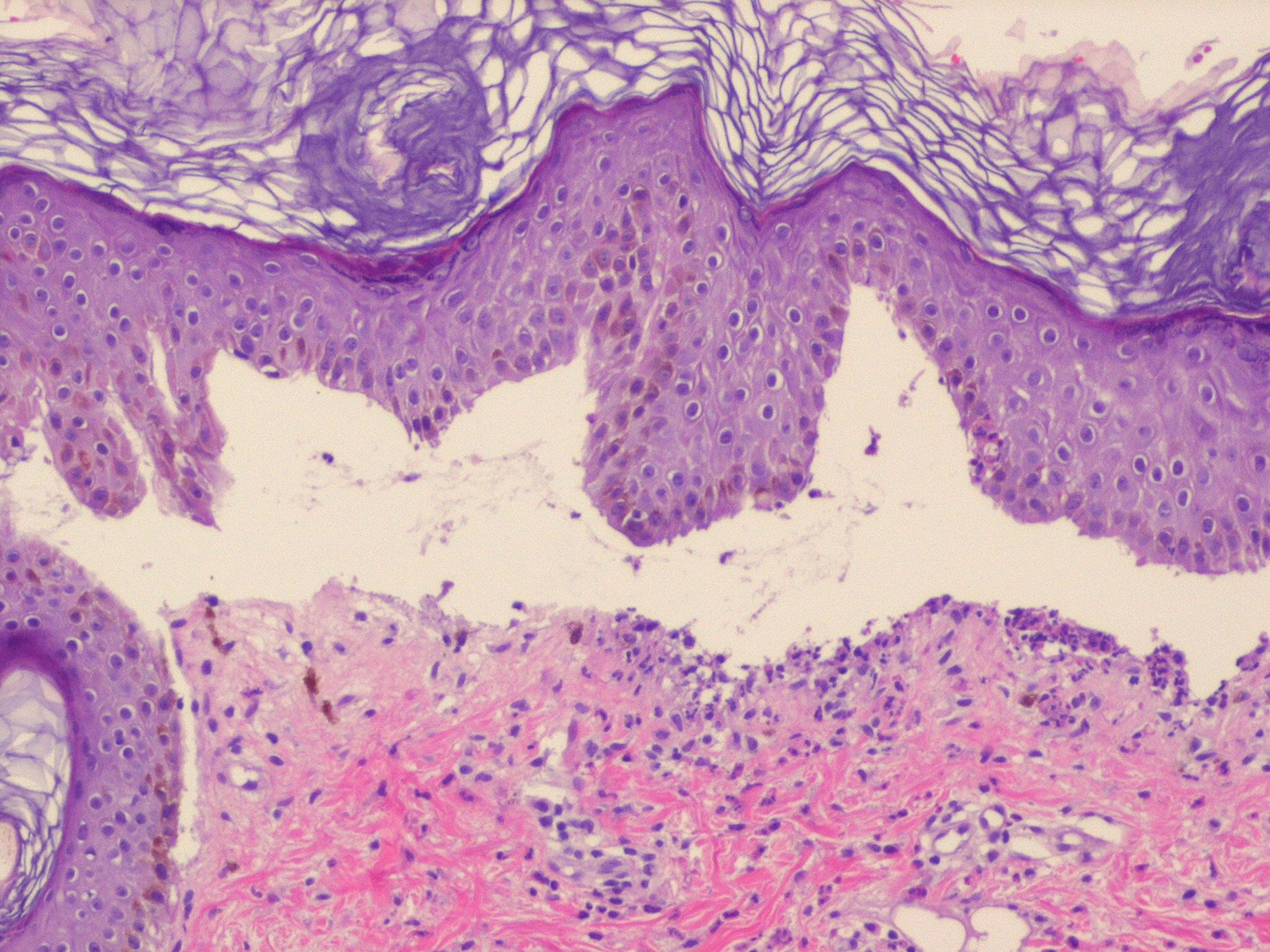
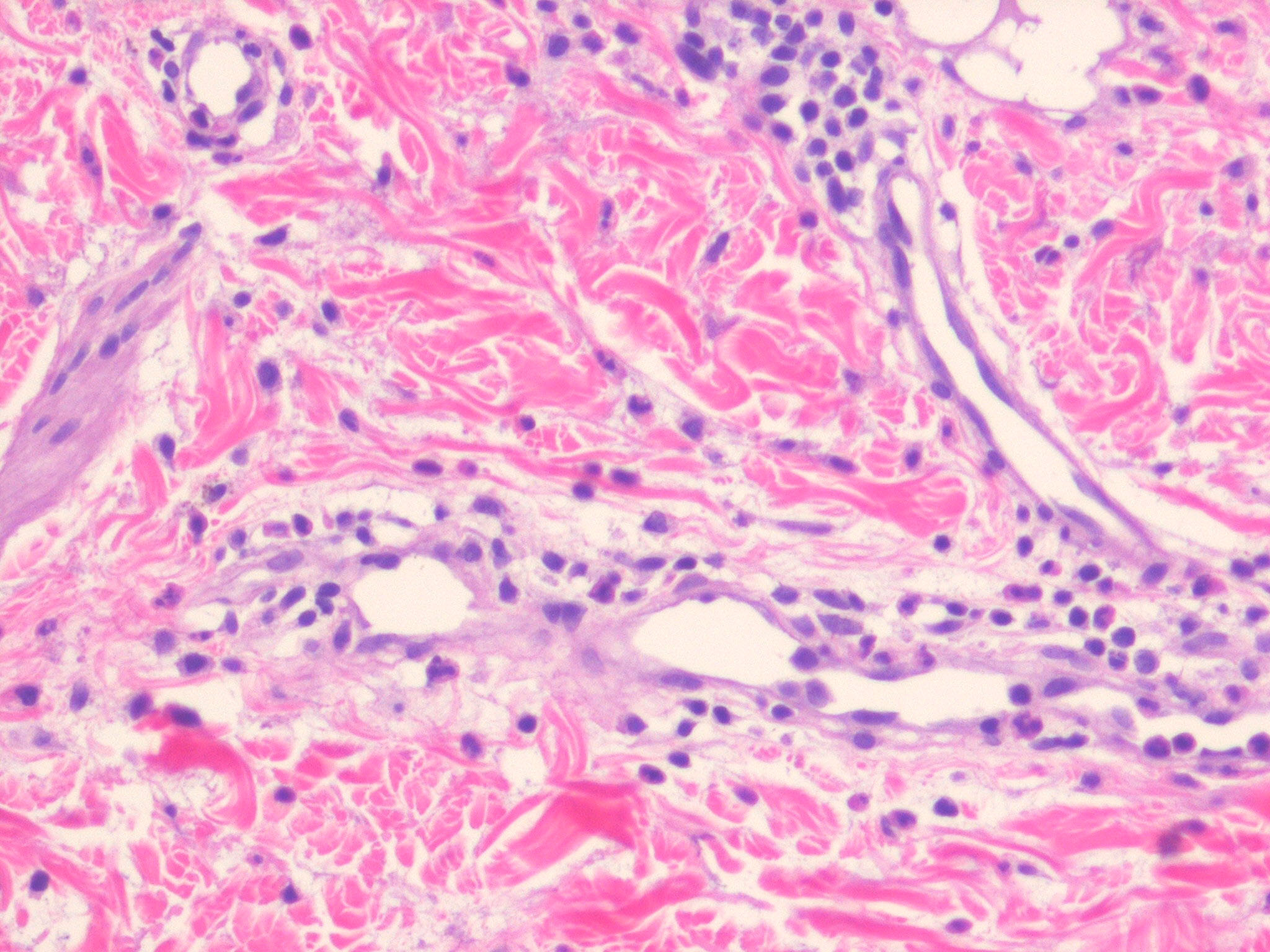
Three histologic patterns have been identified in such lesions. The first is striking basal layer vacuolization with subsequent blister formation. The second is vasculitis with subepidermal blister and pustule formation . The third and most common is a dermatitis herpetiformis-like histologic pattern. Approximately 25% of
|
|
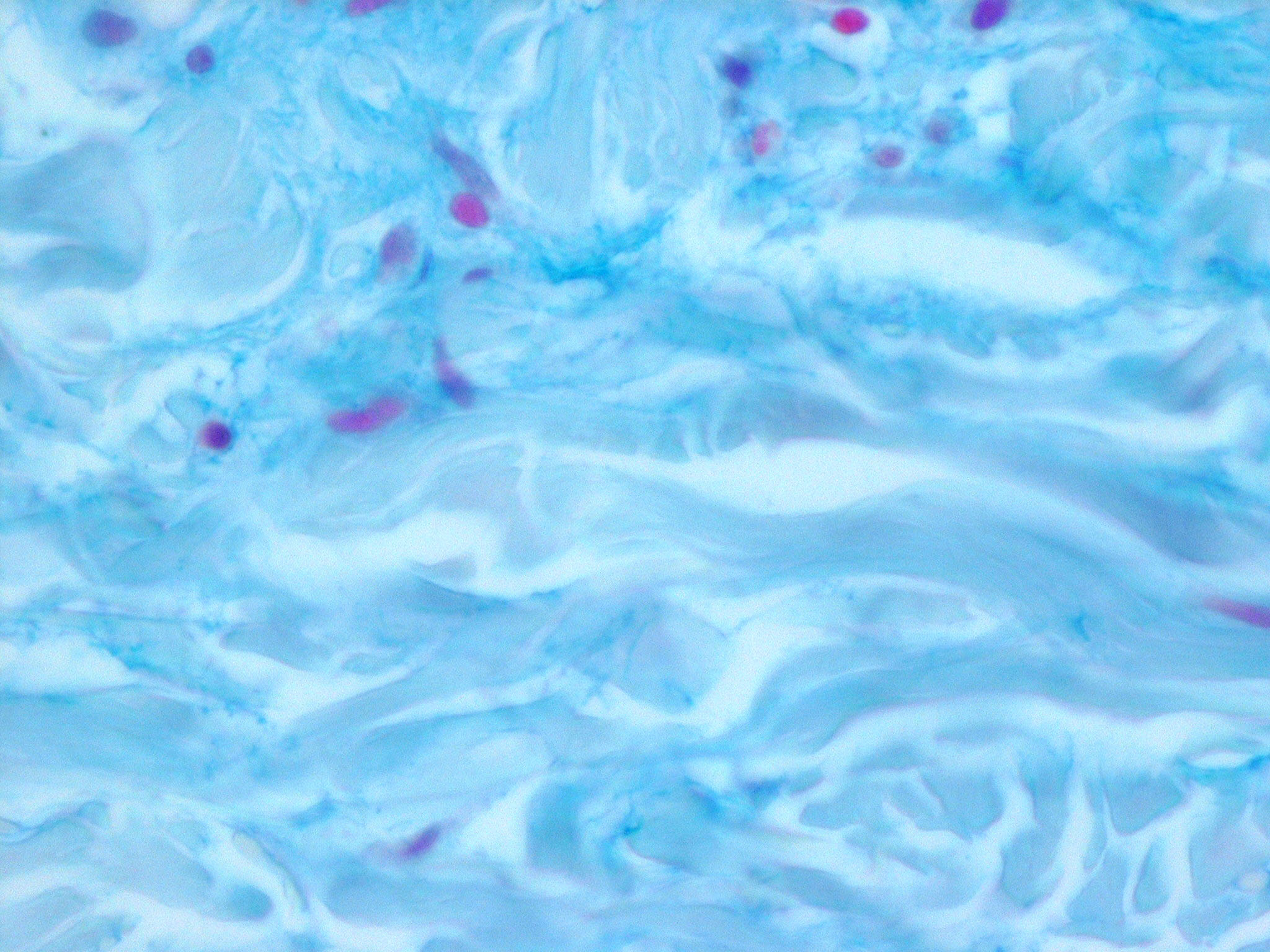
cases are said to have a small-vessel, neutrophil-rich leukocytoclastic vasculitis beneath the blister. Histologic features more routinely identified with lupus erythematosus are not present. Another histologic finding that is not emphasized in most case reports is the presence of dermal mucin and hyaluronic acid as defined by Alcian blue stain at pH 2.5 . The frequency of mucin deposition is unknown.
|
|
IF Testing. In all reported cases, IgG and C3 are deposited at the epidermal basement membrane zone. The pattern was linear in more than 50% and was referred to as "granular band like" in approximately 25%. IgM and IgA were present in approximately 50% and 60% of cases, respectively. The conflicting pattern of immune reactant deposition is difficult to explain. In these reports, the pattern varies from a "thick band" to a "fine ribbon-like" or "tubular" pattern. The ribbon-like or linear pattern represents antibodies that are bound to rigid, anatomically compartmentalized antigens such as in bullous pemphigoid or EBA. In general, granular patterns represent deposition of circulating immune complexes in situ or in situ binding of antigen and antibody in noncompartmentalized zones. Therefore, perhaps some of the cases represent tubular or linear deposition obscured by confluent granular bands (positive lupus band test). IIF study of serum rarely reveals circulating antisquamous basement membrane zone antibodies that are detected against type VII collagen. It should be noted, however, that salt-split skin preparations might be a more sensitive substrate than whole-skin mounts.
|
|
A salt-split skin preparation using patient serum reveals localization to the split floor, as in EBA . As well, Western immunoblot reveals binding to 290-kD or 145-kD dermal proteins, which are components of type VII collagen. However, antibodies to type VII collagen are not present in all cases.
|
|
Ultrastructural Study
. lmmunoelectron microscopic examination reveals electron-dense deposits of IgG at the lower edge of the basal lamina and immediately subjacent dermis in an identical location to the antibody in EBA.
|
|
cases are said to have a small-vessel, neutrophil-rich leukocytoclastic vasculitis beneath the blister. Histologic features more routinely identified with lupus erythematosus are not present. Another histologic finding that is not emphasized in most case reports is the presence of dermal mucin and hyaluronic acid as defined by Alcian blue stain at pH 2.5 . The frequency of mucin deposition is unknown.
|
|
IF Testing. In all reported cases, IgG and C3 are deposited at the epidermal basement membrane zone. The pattern was linear in more than 50% and was referred to as "granular band like" in approximately 25%. IgM and IgA were present in approximately 50% and 60% of cases, respectively. The conflicting pattern of immune reactant deposition is difficult to explain. In these reports, the pattern varies from a "thick band" to a "fine ribbon-like" or "tubular" pattern. The ribbon-like or linear pattern represents antibodies that are bound to rigid, anatomically compartmentalized antigens such as in bullous pemphigoid or EBA. In general, granular patterns represent deposition of circulating immune complexes in situ or in situ binding of antigen and antibody in noncompartmentalized zones. Therefore, perhaps some of the cases represent tubular or linear deposition obscured by confluent granular bands (positive lupus band test). IIF study of serum rarely reveals circulating antisquamous basement membrane zone antibodies that are detected against type VII collagen. It should be noted, however, that salt-split skin preparations might be a more sensitive substrate than whole-skin mounts.
|
|
A salt-split skin preparation using patient serum reveals localization to the split floor, as in EBA . As well, Western immunoblot reveals binding to 290-kD or 145-kD dermal proteins, which are components of type VII collagen. However, antibodies to type VII collagen are not present in all cases.
|
|
dermis in an identical location to the antibody in EBA.
|
|