▪ ANGIOSARCOMA
Epidemiology and Pathogenesis
Angiosarcomas are highly malignant vascular tumors with an incidence of approximately 0.01/100,000 affecting primarily adult patients.88 They may occur in different organs but in more than 50 percent localize to the skin of the head and neck regions.89,90 Besides primary tumors, which appear in previously normal skin, angiosarcomas show an increased incidence in skin with chronic lymphedema, most frequently, but not exclusively, after mastectomy with lymph node dissection. This variant is also referred to as Stewart-Treves syndrome91 and was formerly classified as lymphangiosarcoma. A rare variant is postirradiation angiosarcoma, which may develop after radiation therapy for mammary carcinoma.92
Tumor cells of angiosarcoma express to varying degrees differentiation markers of both the lymphatic and vascular endothelial cell lineage.93 Whether common precursor cells (i.e., angioblasts) give rise to the tumor cells remains to be seen. Therefore, the designation angiosarcoma instead of either lymphangiosarcoma or hemangiosarcoma seems appropriate at the moment. In contrast to KS, angiosarcoma is usually negative for HHV-8.
Clinical Manifestations
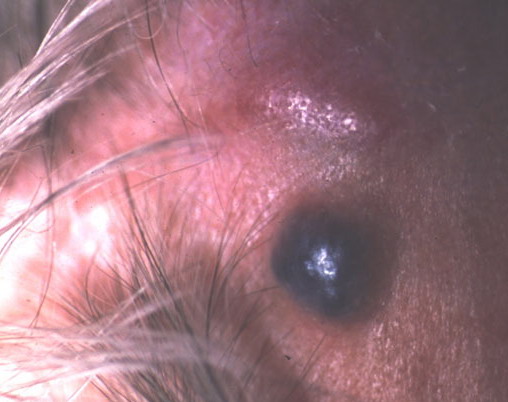
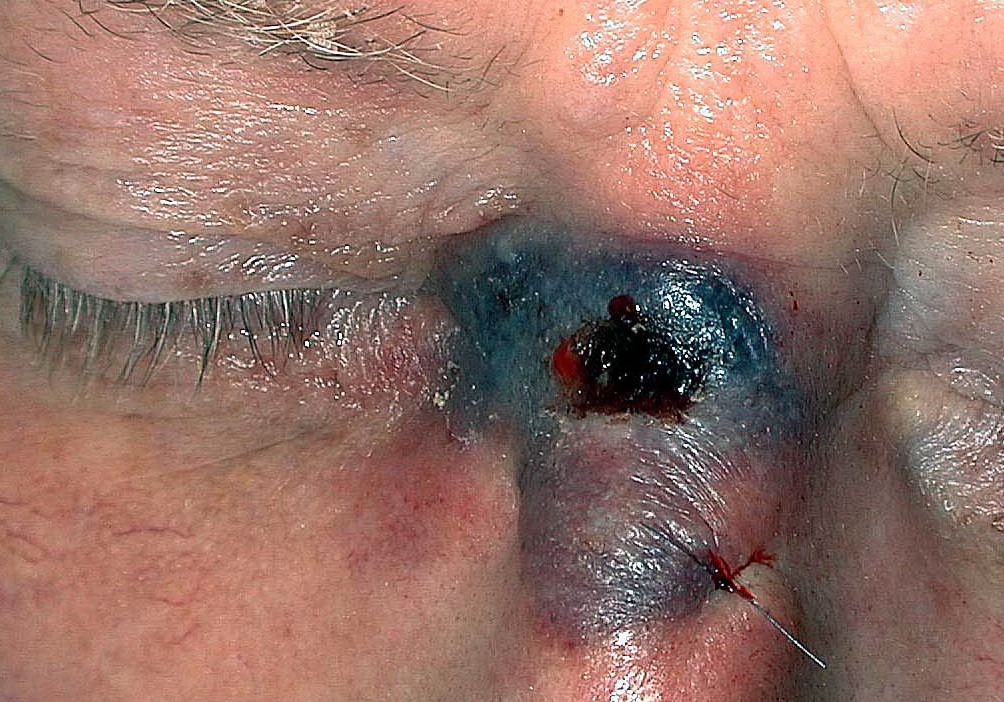
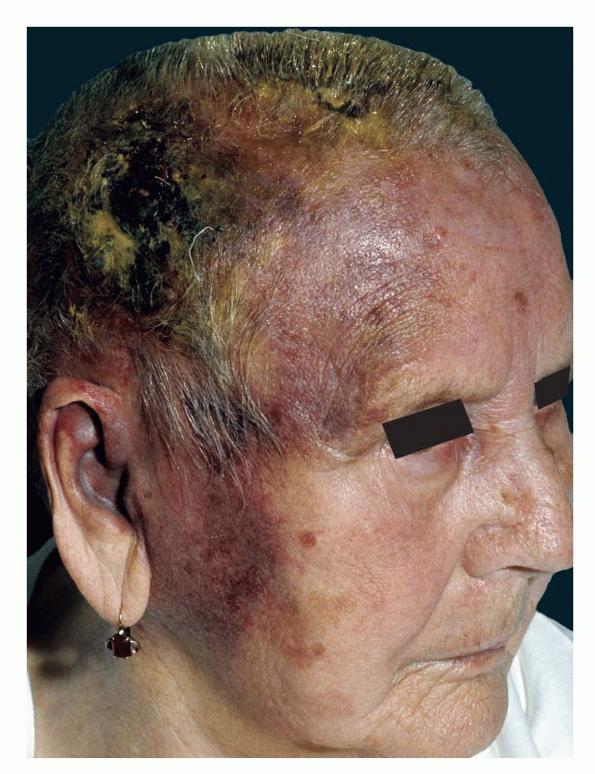
Initially, primary angiosarcoma of the skin presents as singular or multifocal “bruise”-like patches on the skin, most frequently on the face , scalp, or neck regions. In the “head-tilt” maneuver, where the patient lowers the head below the level of the heart, the involved skin becomes deeper red and violaceous and painful throbbing may be felt.94 On progression, the lesions become violaceous and ill-defined spongy nodular tumors appear, which bleed easily. Horizontal spread can lead to the involvement of large skin portions . The tumor
usually progresses along the vascular structures of the neck (see eFig. 128-7.1 in on-line edition) to the mediastinum but distant metastases also occur. Prognosis is poor. Angiosarcoma developing in chronic lymphedema [i.e., Stewart-Treves syndrome (Fig. 128-8) as well as post-irradiation angiosarcoma ] arises as infiltrating hemorrhagic plaques or violaceous nodules accompanied by edema. They are also high-grade malignancies with a poor prognosis.
Differential Diagnoses
Early lesions can be confused with various skin pathologies with vascular involvement including ecchymoses, port-wine stain, rosacea, and early KS. For advanced tumors, pyogenic granuloma, lymphoma, and amelanotic melanoma, cutaneous metastasis of internal malignancies have to be considered.
Hlstopathology
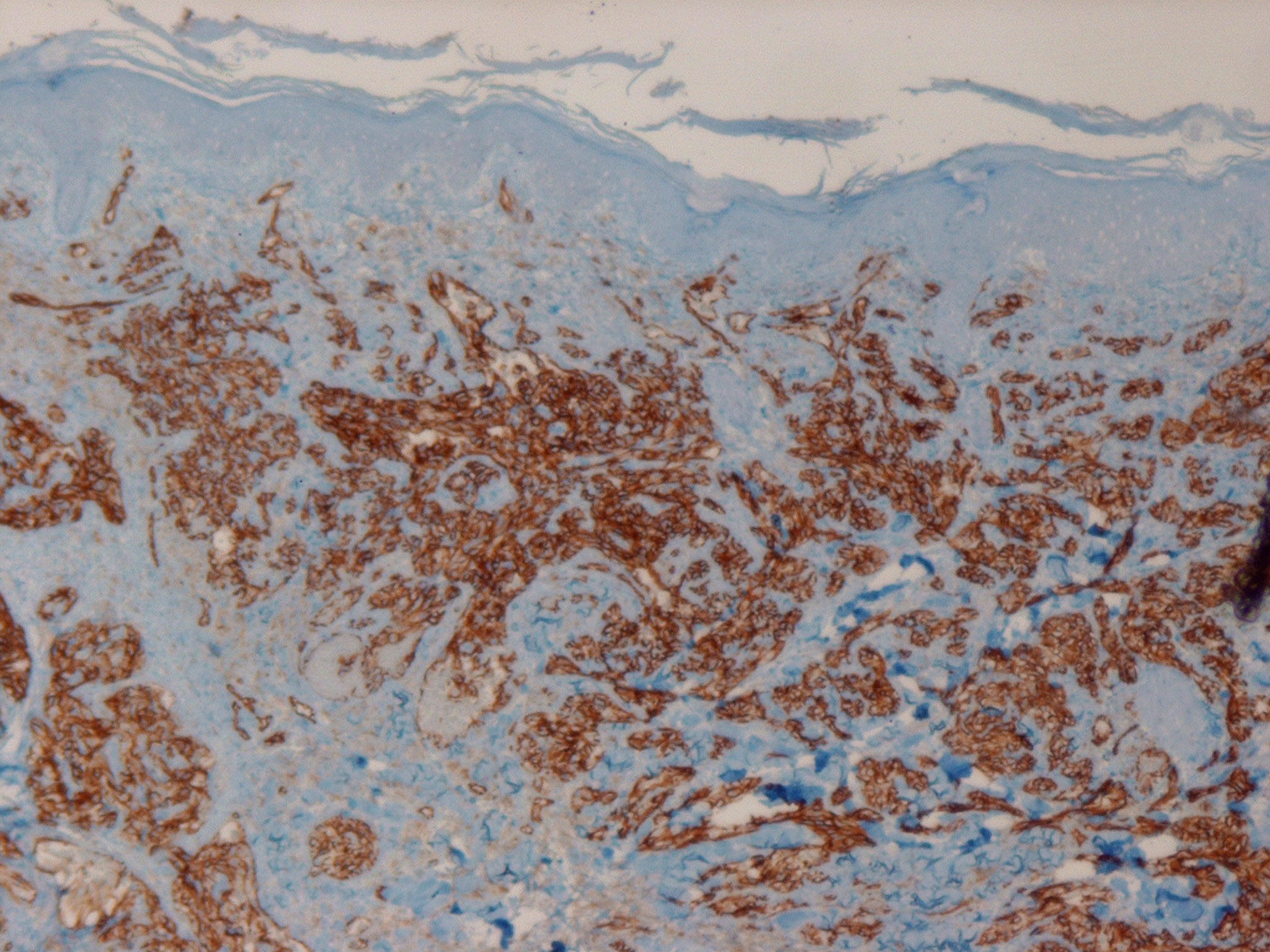
The different clinical variants are indistinguishable histologically and great variability with regard to differentiation of vascular elements can be seen even within individual lesions. Irregular, anastomosing vascular channels lined by endothelial cells with different degrees of atypia and mitotic activity may alternate with areas of closely packed cells with a high mitotic index and sometimes spindle-like morphology . In the latter, less well-differentiated areas and little or no luminal differentiation is present. In particular, in these instances immunostaining for vascular markers such as CD31 and CD34 is helpful for the establishment of the diagnosis.
Treatment
Current treatment is not highly effective with an overall estimated 5-year survival of 15 percent. Due to the rarity of angiosarcomas, comparative therapeutic trials are not available. Treatment of choice for small tumors is excision with wide margins. When surgery is not an option, palliative radiotherapy or chemotherapy should be considered. Both liposomal doxorubicin and paclitaxel were recently demonstrated to be of benefit for patients with widespread disease. Interferon-α, although not effective by itself, holds some promise in combination with either doxorubicin or 13-cis retinoic acid.