|
Aphthosis Behcet s Disease
Behcet's disease is a symptom complex of oral and genital ulceration and iritis that has a worldwide distribution but is most common in the Pacific rim and eastern Mediterranean (. The presence of oral ulceration plus any two signs of genital ulceration, skin lesions (e.g., pustules or nodules), or eye lesions (e.g., uveitis or retinal vasculitis) is diagnostic.
|
|
The cutaneous lesions include erythema nodosum-like nodules, vesicles, pustules, pyoderma gangrenosum, Sweet's syndrome, a pustular reaction to needle trauma, superficial migratory thrombophlebitis, ulceration, infiltrative erythema, acral purpuric papulonodular lesions, and acneiform folliculitis .
|
|
The extracutaneous manifestations are categorized as oral and/or genital aphthae; vasculo-, ocular-, entero-, or neuro-Behcet's disease; renal disease; and arthritis. Oral apthosis recurring at least three times over a 12-month period is essential to the diagnosis . In vasculo-Behcet's disease, aneurysms and occlusive venous and arterial main vessel lesions occur. The ocular manifestations include uveitis, hypopyon iritis, optic neuritis, and choroiditis. Entero-Behcet's disease manifests as diarrhea, constipation, abdominal pain, vomiting, and melena. Neuro-Behcet's disease presents as brainstem dysfunction, meningoencephalitis, organic psychiatric symptoms, and mononeuritis multiplex . Asymptomatic microhematuria and/or proteinuria are among the renal manifestations. An oligoarthritis may involve the wrist, elbow, knee, or ankle joints. Morbidity and mortality in one large series of Turkish patients were greatest in young males; both the onset and the severity of ocular disease were greatest early in the course of disease, suggesting that the "disease burden" in Behcet's disease is greatest early and that it tends to "burn out" over time . However, neurologic and major vessel disease can occur at any time and can have late onset 5 to 10 years into the course of illness .
|
|
Histopathology
The cutaneous lesions can be categorized histopathologically into two main groups: vascular and extravascular with or without vasculopathy including acneiform.
|
|
The pathologic spectrum of the cutaneous vasculopathy encompasses a mononuclear cell vasculitis with variable mural and luminal fibrin deposition; a paucicellular thrombogenic vasculopathy ; and a neutrophilic vascular reaction involving capillaries and veins of all calibers. The mononuclear cell reaction may be frankly granulomatous or it may be lymphocytic predominant to define a lymphocytic vasculitis. The neutrophilic vascular reaction may resemble that of Sweet's syndrome or a leukocytoclastic vasculitis. Diffuse extravascular mononuclear cell- and/or neutrophil-predominant inflammation of the dermis and/or panniculus may occur with or without the aforementioned vascular changes. The histiocytes infiltrating the panniculus may manifest phagocytosis of cellular debris. Suppurative or mixed suppurative and granulomatous folliculitis with or without
|
|
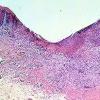
Extracutaneous lesions histologically mirror the skin changes. Oral aphthous ulcers demonstrate a central diffuse
|
|
neutrophilic infiltrate with necrosis of the epithelium and connective tissue pathergy of the submucosa and peripherally a border showing dense lymphocytic infiltration with lymphocytic exocytosis and degenerative epithelial changes. Genital aphthae have the same appearance . The large-vessel arteriopathy represents an ischemic sequelum of a mononuclear cell vasculitis of the vasa vasorum , whereas venous thrombosis may be due in part to an underlying hypercoagulable state. A lymphocytic vascular reaction with or without mural and intraluminal fibrin deposition is the histopathology of neuro-, entero-, ocular-, and arthritic Behcet's disease, with other organ changes such as demyelination and intestinal ulceration reflecting resultant ischemia . The renal histopathology includes IgA nephropathy, focal and diffuse proliferative glomerulonephritis, and amyloidosis .
|
|
Differential Diagnosis.
The lymphocytic vasculitis observed in Behcet's disease may mimic that seen in association with systemic lupus erythematosus, rheumatoid arthritis , Sjogren's syndrome, relapsing polychondritis, Degos' disease, and paraneoplastic vasculitis in the setting of Iymphoproliferative disease. Granulomatous vasculitis may also be observed in Wegener's granulomatosis, allergic granulomatosis of Churg-Strauss, Crohn's disease, sarcoidosis, acquired hypogammaglobulinemia, a postherpetic eruption , paraneoplastic syndrome (related to underlying hematologic malignancy), rheumatoid arthritis, hypersensitivity reactions to certain infections including syphilis and tuberculosis , scleroderma, and late-stage lesions of microscopic polyarteritis nodosa . Other causes of a Sweet's-like vasculopathy include Sweet's syndrome, bowel arthritis dermatosis, pyoderma gangrenosum, and idiopathic pustular vasculitis . Conditions that combine a vasculitis with a folliculitis include pyoderma gangrenosum, mixed cryoglobulinemia, rheumatoid vasculitis, and bacterid .
Pathogenesis
An immunogenetic basis is likely in view of the association with certain HLA types, namely HLA-B5, HLA-B12, HLA-B27, and HLA-B51 . A recurring association in patients of Japanese, Turkish, Korean, and Iranian ethnicities is with HLA-B51 (115, 116), genetic polymorphisms in the promoter region of tumor necrosis factor-a (TNFa) .and microsatellite instabilities between these two genes . Polymorphisms of other cytokines have been identified, including IL-1 and IL-18 . Behcet's disease patients have elevated levels ofTh1 cytokines IL-12, IFNy, and TNFa ; increased Th1-associated chemokine receptors CCR5 and CXCR3 , and a lower percentage of plasmacytoid dendritic cells in peripheral blood , supporting the proposed Th1-mediated pathogenesis of the disease. Patients have shown a heightened immune response to antigenic components of certain streptococcal species , Mycobacterium tuberculosis , herpes simplex , Epstein-Barr virus, and human immunodeficiency virus (HIV) . Underlying abnormalities in T-Iymphocyte function may be integral to an aberrant response related to the synthesis by microorganisms and mammalian tissue of a family of polypeptides termed heat shock proteins (HSPs) produced by cells exposed to stresses such as increased temperature. Sensitized T cells and T-cell clones specific to the 65-kD mycobacterial HSP have been reported in rheumatoid arthritis . T lymphocytes from patients with Behcet's disease in one study exhibit a greater stimulation by this HSP compared to normal controls or patients with unrelated disease . The yfJ T-cell subset has been shown to be the principal populace that responds to the mycobacterial 65-kD HSP, an observation that may account for the increase in circulating yfJ T cells in patients with antecedent streptococcal or mycobacterial infections and in those with active Behcet's disease, in whom an exaggerated response to microbial products in mucosal ulcers is postulated (138). The lymphocytes themselves show resistance to Fas-mediated apoptosis, a finding that may promote lymphocyte-mediated tissue destruction in these patients .
Tissue neutrophilia may relate to the presence of HLA-B51, which has been associated with neutrophil hyperreactivity . Neutrophil functions are also increased in Behcet's disease , which may be due to alteration in expression of Toll-like receptors, regulators of innate and adaptive immunity, on both granulocytes and monocytes .
|
|
Vascular thrombosis has been attributed to antibody-mediated endothelial injury , protein Cor S deficiency , factor XII deficiency, inhibition of plasminogen activator, and circulating lupus anticoagulant . A prothrombin gene mutation has recently been described . Further evidence of a genetic predisposition to thrombosis is the linkage of HLA-B51 expression and the absence of HLA-B35 as risk factors for venous thrombosis in Turkish patients ; there is also a statistical linkage between superficial and deep venous thrombosis . Elevated serum levels of matrix metalloproteinases MMP-2 and MMP-9 are associated with vasculo-Behcet's disease, particularly thrombotic and aneurysmatic involvement, respectively .
|
|
vasculitis characterizes the acneiform lesions. Acral purpuric papulonodular lesions show a lymphocytic interface dermatitis with lymphocytic exocytosis, dyskeratosis, and a perivascular lymphocytic infiltrate, recapitulating the mucosal histopathology .
|
|
The role of nitric oxide (NO) is unclear. Some researchers have shown that patients with active Behcet's disease have significantly higher serum levels of NO than patients with recurrent aphthous stomatitis , patients with inactive Behcet's disease, and healthy controls , whereas others maintain that there is no difference in NO levels among these groups , and still others contend that levels of NO are lower in Behcet's patients . Specific genetic polymorphisms have been identified in the manganese superoxide dismutase gene in Japanese Behcet's patients and the Glu298Asp polymorphism in the endothelial nitric oxide synthase (eNOS) gene in Turkish , Italian , and Korean Behcet's patients. One study did not identify the eNOS polymorphism in Turkish Behcet's patients . Others propose that the significantly higher levels of IL-2, IL-6, TNFa, and NO are related to the pathogenesis of Behcet's disease .
|
|
|
|
|





