Congenital Onychodystrophy of the Index Fingers
Congenital onychodystrophy of the index fingers (COIF), a term Kikuchi et al coined in 1974 identifies a clinical syndrome consisting of nail dysplasias of the index fingers associated with underlying bone abnormalities. The first case report of this condition is attributed to Kamei. Iso collected a series of patients with this condition and made the first attempt to define the clinical syndrome. Kikuchi et al observed additional variations in the manifestations of the nail dysplasia and noted the associated radiographic abnormalities of the distal phalanges of the index fingers. The spectrum of underlying bone abnormalities has since been expanded to include the following:
- A Y-shaped bifurcation of the distal phalanx on lateral view
- Narrowing and terminal enlargement of the distal phalanx on anteroposterior view
- Brachymesophalangia (shortening of the middle phalanx of the fifth digit)
- Syndactyly of the index and other fingers
The clinical spectrum of nail abnormalities has expanded to include malalignment and deformities of nails other than the nails of the index fingers.
Although no evidence from the Iso's series indicates hereditary transmission of congenital onychodystrophy of the index finger, Millman and Strier reported a 5-generation family in which 9 individuals had congenital onychodystrophy of the index finger.4 The investigators observed an autosomal dominant pattern of inheritance with variable penetrance.
If data from small series, case reports, and retrospective reviews over 30 years are summarized, the 4 cardinal features of congenital onychodystrophy of the index finger are the following:
- Unilateral or bilateral hypoplasia of the index fingernails
- Deformities of the nails on other fingers
- Radiographic abnormalities of the distal bony phalanx on the affected fingers
- Congenital occurrence, which can be either hereditary or sporadic
A genetic mechanism most likely underlies the pathophysiology of congenital onychodystrophy of the index finger. Two other proposed theories are (1) in utero ischemic injury and (2) in utero exposure to teratogens.
In utero ischemic injury
On the basis of 2 cases of syndactyly associated with digital artery hypoplasia and another case of traumatic injury leading to arterial hypoplasia and permanent nail loss, Kitayama and Tsukada proposed that congenital onychodystrophy of the index finger is due to in utero ischemic injury.5 Kikuchi proposed that ischemia occurs because of an abnormal fetal grip in which the thumbs are pressed on the index fingers during the critical period in the development of the distal phalanx and nail.
Although the association of ischemic injury and nail malformation is of considerable interest, the abnormal grip theory is not consistent with our understanding of human developmental biology. Bones are mesodermal derivatives, and limbs are the result of the apical ectodermal ridge exerting an inductive influence on limb mesenchyme. This development occurs early in fetal life and therefore seems to exclude the possibility Kikuchi suggested, that is, a grip of the fingers from the fetus causes malformation. Such bony malformations would most likely be present prior to the fetus' ability to grip.
In utero exposure to teratogens
Franceschini et al reported a boy with bilateral hypoplasia of the index fingers associated with mild mental retardation, inguinal hernia, macrocephaly, medial flaring of the eyebrows, esotropia of the left eye, long palpebral fissures, malar hypoplasia, a high-arched palate, clinodactyly of the fifth fingers, and a simian palmar crease.6 Radiographs of the hands revealed a hypoplastic terminal tuft on both index fingers. They reported this case as congenital onychodystrophy of the index finger and suggested that the other associated anomalies expanded the definition of the congenital onychodystrophy of the index finger syndrome.
Although maternal exposure to antiepileptic drugs (AEDs) was not specifically mentioned in this case report, the findings are consistent with fetal AED syndrome, and, in fact, hypoplasia of the distal digits is a well-recognized finding in the broad spectrum of fetal AED syndrome. The teratogenicity of AEDs is probably related to either their antifolate effects or the metabolic generation of toxic metabolites such as epoxides (arene oxides), especially in individuals who lack epoxide hydrolase. Although no data link in utero AED exposure to the narrow spectrum of congenital onychodystrophy of the index finger, other, as yet unidentified, in utero exposures remain a possible cause of the genetic damage that allow expression of congenital onychodystrophy of the index finger, especially in mothers with epoxide hydrolase deficiency.
The true prevalence of congenital onychodystrophy of the index fingers in the United States is unknown.
Most case reports of congenital onychodystrophy of the index finger are from Japan, but whether this predominance is due to increased awareness of the syndrome in Japan or actual prevalence is unclear. A 2008 case report is from Brazil, which may be the first case of congenital onychodystrophy of the index finger reported from South America.7 An Israeli registry that monitors all congenital anomalies included 3 cases among approximately 71,000 live births between 1977 and 1997 (4.2 cases per 100,000 live births). Whether this rate is accurate for other areas of the world is unknown.8
Congenital onychodystrophy of the index finger is not associated with mortality or significant morbidity.
Most case reports of congenital onychodystrophy of the index fingers are from Japan. However, whether Japanese individuals are affected more often than others or whether Japanese clinicians are simply more aware of congenital onychodystrophy of the index finger syndrome than others (given where the syndrome was first identified) is unclear. Cases have also been reported in whites and in people of East Indian descent.
Both sexes are equally affected by congenital onychodystrophy of the index fingers.
Congenital onychodystrophy of the index fingers is congenital.
Congenital onychodystrophy of the index fingers is congenital.
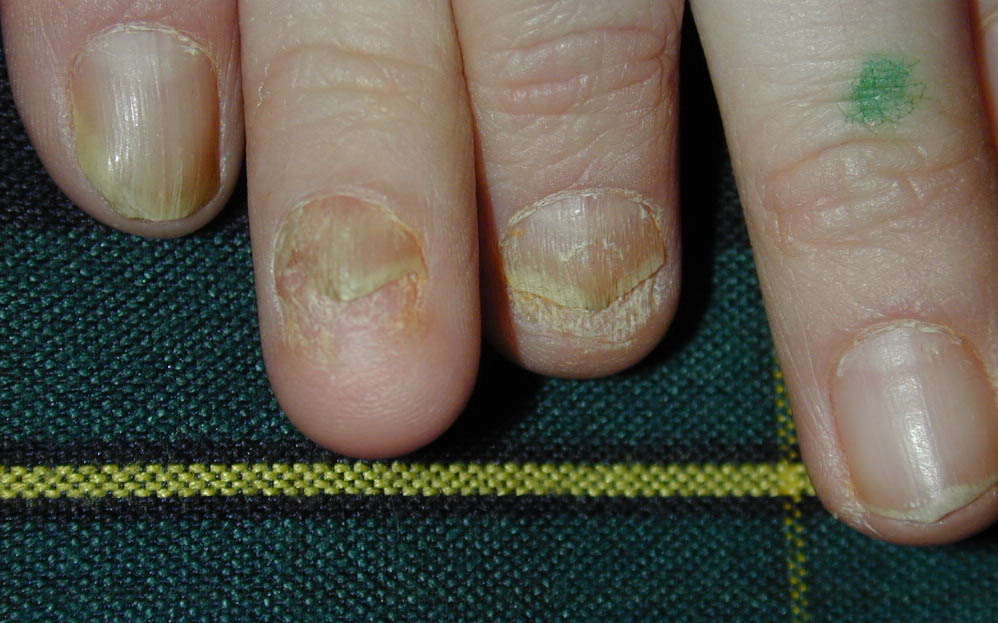
Various nail abnormalities are observed, including (1) anonychia (lack of a fingernail), (2) micronychia (a small fingernail deviated to 1 side of the nail bed), (3) polyonychia (multiple, small, individual nails on one nail bed), (4) hemionychogryphosis (partial thickening and curvature of the fingernail), and (5) irregular lunula and nail malalignment. Appearance is displayed in the image below.
Micronychia is the most common clinical manifestation of congenital onychodystrophy of the index finger. This differs from the usual form of micronychia, which is located on the central part of the finger. In the micronychia of congenital onychodystrophy of the index finger, the onychodysplasia is deviated to the radial aspect of the involved digits. Additionally, most commonly, the index finger is involved, either unilaterally or bilaterally. Involvement of other fingers and toes is also reported. A 2008 case report describes a patient with congenital onychodystrophy of the index finger who had metacarpal bone abnormalities and no ring finger.
The true cause of congenital onychodystrophy of the index finger remains obscure. However, some evidence supports hereditary transmission. Also possible is an unidentified in utero exposure to teratogens in genetically predisposed individuals, allowing expression of congenital onychodystrophy of the index finger. See Differentials below for similar conditions and distinguishing features.