|
Calcinosis Cutis = الكلاس الجلدي |
 |
 |
 |
|
There are four forms of calcinosis cutis: metastatic calcinosis cutis, dystrophic calcinosis cutis, idiopathic calcinosis cutis, and subepidermal calcified nodule.
|
|
Metastatic Calcinosis Cutis
|
|
Metastatic calcification develops as the result of hypercalcemia or hyperphosphatemia. Hypercalcemia may result from (a) primary hyperparathyroidism, (b) excessive intake of vitamin D , (c) excessive intake of milk and alkali , or (d) extensive destruction of bone through osteomyelitis or metastases of a carcinoma . Hyperphosphatemia occurs in chronic renal failure as the result of a decrease in renal clearance of phosphorus and is associated with a compensatory drop in the serum calcium level. The low level of ionized calcium in the serum stimulates parathyroid secretion, leading to secondary hyperparathyroidism and to resorption of calcium
and phosphorus from bone. The demineralization of bone causes both osteodystrophy and metastatic calcification .
|
|
Metastatic calcification most commonly affects the media of the arteries and the kidneys. In addition, other visceral organs, such as the myocardium, the stomach, and the lungs , may be involved.
|
|
Metastatic calcification in the subcutaneous tissue is occasionally observed in association with renal hyperparathyroidism , in uremia , in hypervitaminosis D , and as the result of excessive intake of milk and alkali but rarely in primary hyperparathyroidism . Palpable, hard nodules, occasionally of
|
|
considerable size, are located mainly in the vicinity of the large joints . With an increase in size, the nodules may become fluctuant .
|
|
Calciphylaxis is a life-threatening condition in which there is progressive calcification of small- and medium-sized vessels of the subcutis often accompanied by necrosis. It most frequently arises in the setting of hyperparathyroidism associated with chronic renal failure. Calciphylaxis is often, but not always, associated with an elevated serum calcium/phosphate product, with other factors, including several glycoproteins (matrix G1a protein and glycopontin) likely playing a role in the development of vascular calcification .
|
|
Clinically, the lesions present as a panniculitis or vasculitis. Bullae, ulcerations, or a livedo reticularis-like eruption can be present . Potential complications of gangrene, sepsis, pancreatitis, and multisystem organ failure contribute to an overall mortality of >60% .
|
|
Instances of cutaneous metastatic calcinosis are rare. Most reports have concemed patients with renal hyperparathyroidism and osteodystrophy. The cutaneous lesions may consist offirm, white papules ; papules in a linear arrangement ; symmetric, nodular plaques ; or papules and nodules from which a granular, white substance can be expressed .
|
|
Mural calcification of arteries and arterioles in the deep dermis or subcutaneous tissue occurs rarely in primary
|
|
hyperparathyroidism but somewhat more frequently in secondary hyperparathyroidism subsequent to renal disease and particularly if subsequent to dialysis for chronic renal disease or to renal allograft . This may lead to occlusion of these vessels and to infarctive ulcerations, especially on the legs.
|
|
Histopathology
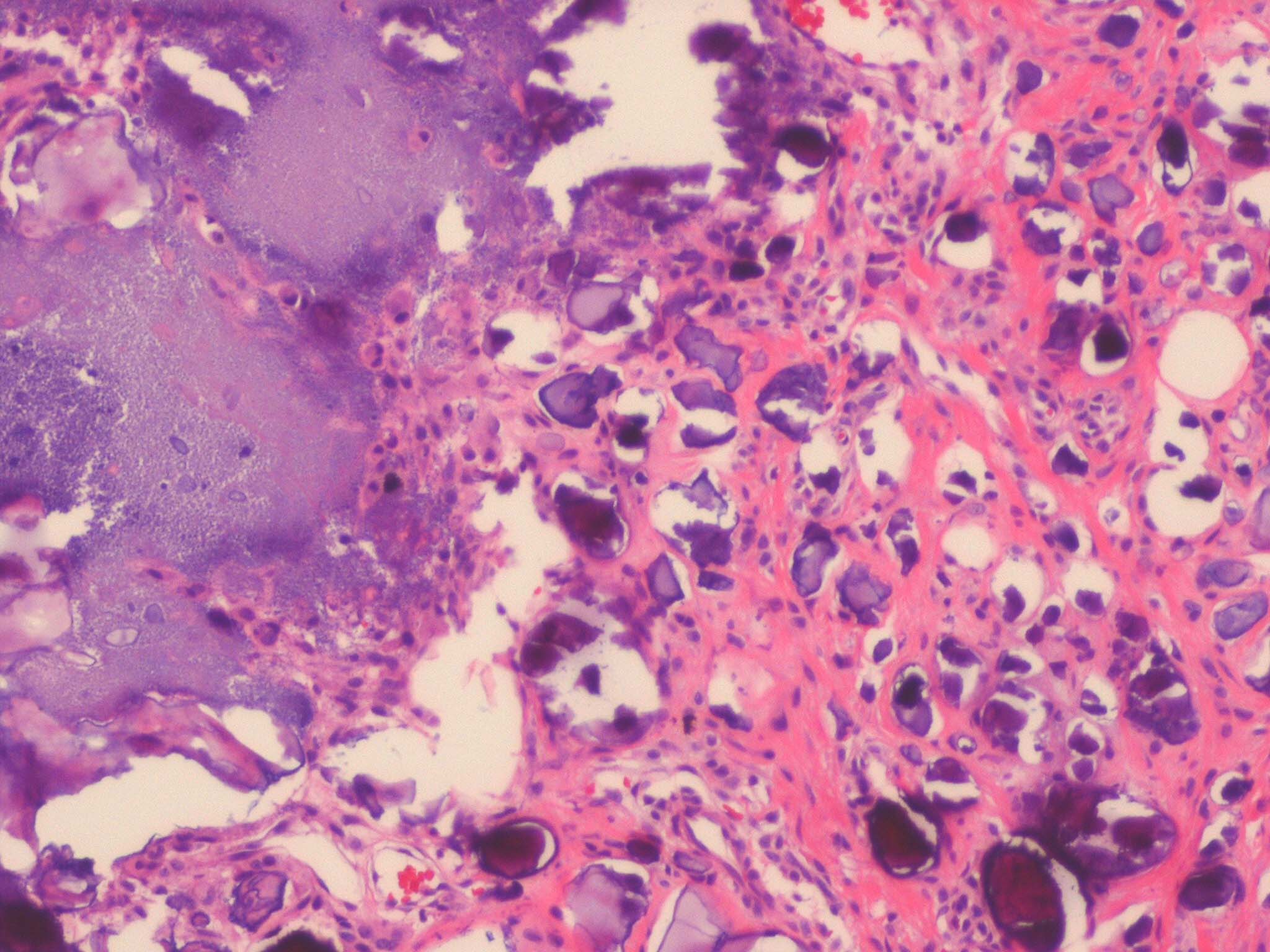
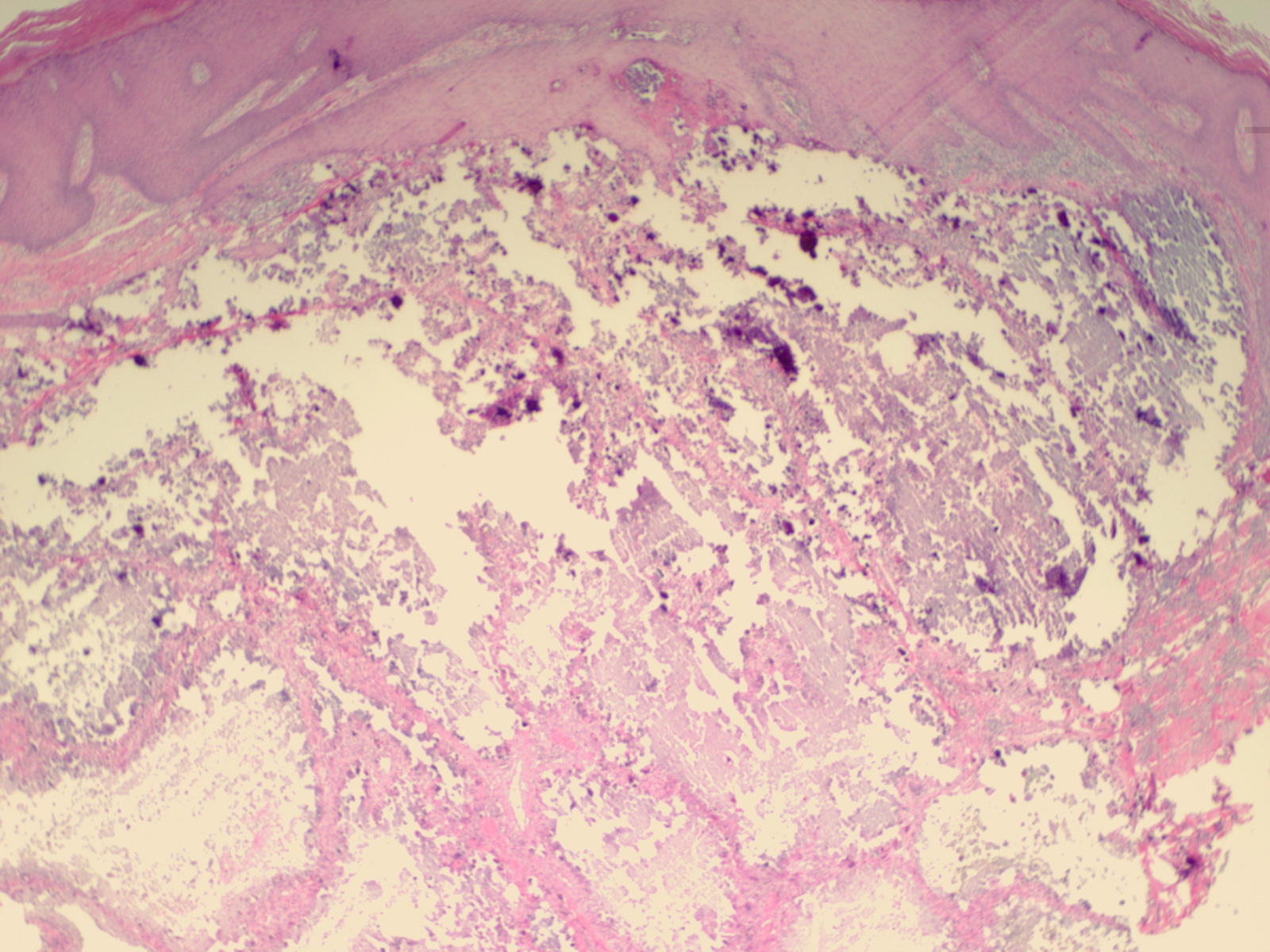
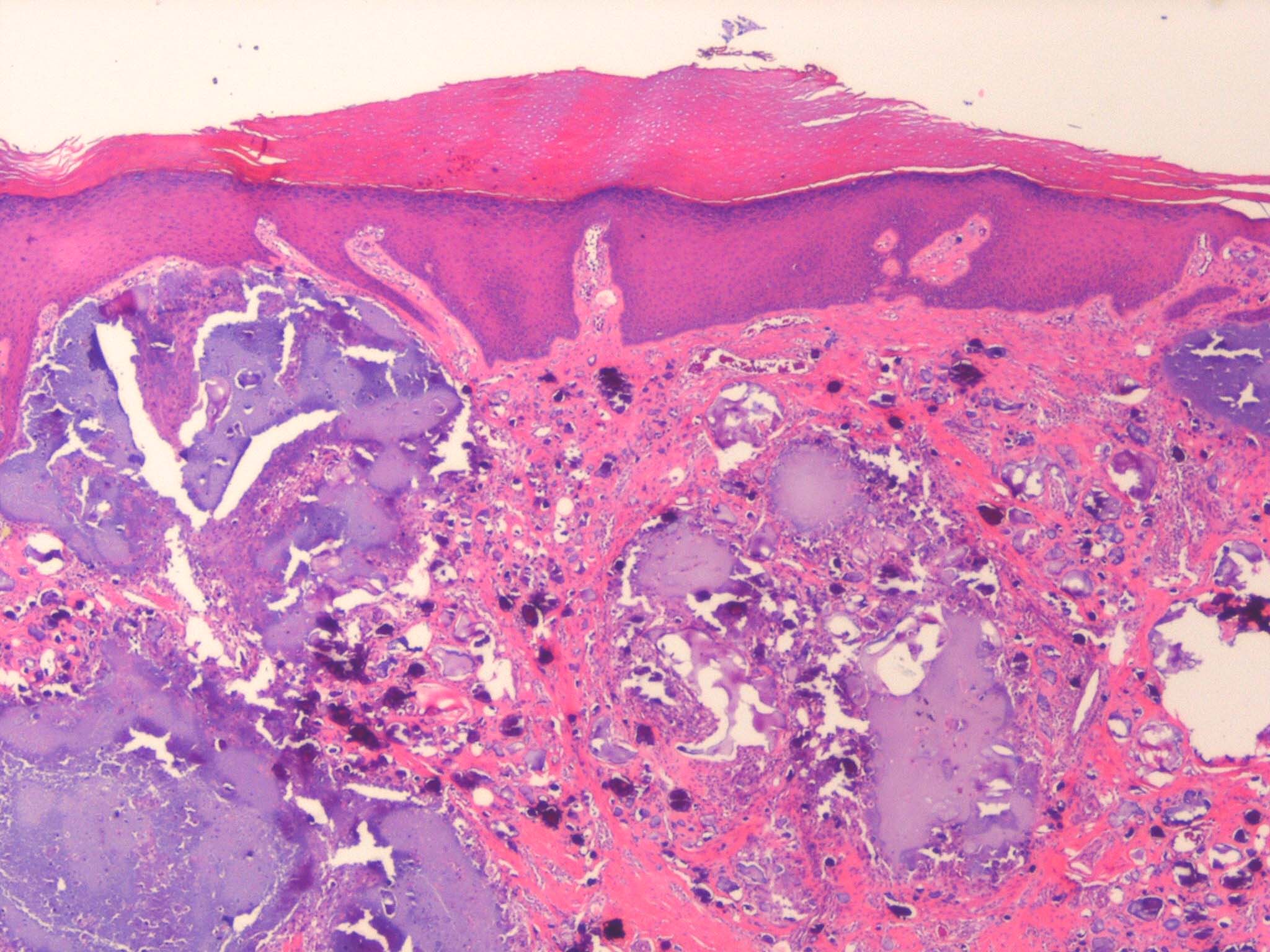
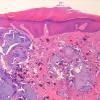
. Calcium deposits are recognized easily in histologic sections, because they stain deep blue with H&E. They stain black with the von Kossa stain for calcium phosphate. As a rule, the calcium occurs as massive deposits when located in the subcutaneous fat and usually as granules and small deposits when located in the dermis (Fig. 17-12). Large deposits of calcium often evoke a foreign body reaction; thus, giant cells, an inflammatory infiltrate, and fibrosis may be present around them .
|
|
In areas of infarctive necrosis, as a result of calcification of dermal or subcutaneous arteries or arterioles, the involved vessels show calcification of their walls and intravascular fibrosis with attempts at recanalization of the obstructed lumina . Mural calcification often is most pronounced in the internal elastic membranes of arteries or arterioles .
|
|
The histologic changes in calciphylaxis include calcium deposits in the subcutis, chiefly within the walls of smalland medium-sized vessels . These deposits can be associated with endovascular fibrosis, thrombosis, or global calcific obliteration . The fully evolved disease process shows, in addition, areas of necrosis with a clean background or accompanied by neutrophils .
|
|
It is particularly important that these findings be recognized in order that appropriate therapy, which often includes parathyroidectomy, might be instituted immediately.
|
|
Dystrophic Calcinosis Cutis
In dystrophic calcinosis cutis, the calcium is deposited in previously damaged tissue. The values for serum calcium and phosphorus are normal, and the internal organs are spared. There may be numerous large deposits of calcium (calcinosis universalis) or only a few deposits (calcinosis circumscripta).
|
|
Calcinosis universalis occurs as a rule in patients with dermatomyositis , but exceptionally it has also been observed in patients with systemic scleroderma . Large deposits of calcium are found in the skin and subcutaneous tissue and often in muscles and tendons . In dermatomyositis, if the patient survives, the nodules of dystrophic calcinosis gradually resolve.
|
|
Calcinosis circumscripta
occurs as a rule in patients with systemic scleroderma; rarely, however, it may be observed in patients with widespread morphea (155, 156). Generally, in the presence of calcinosis, systemic scleroderma manifests itself as acrosclerosis. The association of acrosclerosis and calcinosis is
|
|
often referred to as the Thibierge-Weissenbach syndrome or as the CREST syndrome, because the manifestations usually consist of calcinosis cutis, Raynaud's phenomenon, esophageal dysfunction, sclerodactyly, and telangiectasia .Patients with this syndrome often have a better prognosis than those with generalized scleroderma or systemic sclerosis. Clinically, calcinosis circumscripta shows successively appearing areas of induration that often break down and extrude white, chalky material.
|
|
Lupus erythematosus is only rarely associated with dystrophic calcinosis cutis . In addition to occurring in the connective tissue diseases, dystrophic calcinosis is often seen in subcutaneous fat necrosis of the newborn and, rarely, in the subcutaneous nodules occurring in Ehlers-Danlos disease.
|
|
Histopathology.
As in metastatic calcinosis cutis, the calcium in dystrophic calcinosis cutis usually is present as granules or small deposits in the dermis and as massive deposits in the subcutaneous tissue . A foreignbody giant cell reaction is often found around large deposits of calcium . The calcium deposits usually are located in areas in which the collagen or fatty tissue appears degenerated as a result of the disease preceding the calcinosis.
|
|
Idiopathic Calcinosis Cutis
|
|
Even though the underlying connective tissue disease in some instances of dystrophic calcinosis cutis may be mild and can be overlooked unless specifically searched for, there remain cases of idiopathic calcinosis cutis that resemble dystrophic calcinosis cutis but show no underlying disease .
|
|
One entity is regarded as a special manifestation of idiopathic calcinosis cutis: tumoral calcinosis. It consists of numerous large, subcutaneous, calcified masses that may be associated with papular and nodular skin lesions of calcinosis . The disease usually is familial and is associated with hyperphosphatemia . Otherwise, the resemblance of tumoral calcinosis to the dystrophic calcinosis universalis observed with dermatomyositis is great.
|
|
Histopathology.
Tumoral calcinosis shows in the subcutaneous tissue large masses of calcium surrounded by a foreign body reaction . Intradermal aggregates are present in some cases. Discharge of calcium may take place through areas of ulceration or by means of transepidermal elimination .
|
|
Pathogenesis
. Two authors have studied lesions of idiopathic calcinosis cutis by electron microscopy (160,161). They agree that the deposits consist of pleomorphic calcium phosphate (apatite) crystals. However, according to one opinion, the earliest deposits of calcium are situated in the ground substance (160), whereas according to the other, the earliest calcium deposits lie within collagen fibrils and subsequently extend into the ground substance as the apatite crystals grow (161 ).
|
|
Idiopathic Calcinosis of the Scrotum
Idiopathic calcinosis of the scrotum consists of multiple asymptomatic nodules of the scrotal skin. The nodules begin to appear in childhood or in early adult life, increase in size and number, and sometimes break down to discharge their chalky contents .
|
|
Histopathology
At one time, the accepted view was that some of the calcific masses in calcinosis of the scrotum were surrounded by a granulomatous foreign body reaction and others were not . However, in recent publications in which numerous scrotal nodules were examined, some of the lesions were epidermal cysts, whereas other cystic lesions showed calcification of their keratin contents, and still others showed ruptures of their epithelial walls. The cyst wall was eventually destroyed, leaving only dermal collections of calcium. Thus,
according to this view, calcinosis of the scrotum represents the end stage of dystrophic calcification of scrotal epidermal cysts . Other authors who also had examined either several patients or multiple nodules agreed that the lesions originated from cysts. One author favored eccrine duct milia as the origin because of a positive reaction for carcinoembryonic antigen, which is a marker of eccrine sweat glands (. Another author found various types of cysts-epidermal, pilar, and indeterminate cysts showing various degrees of calcification . It can be assumed that early lesions start out as cysts but, as they age and calcify, lose their cyst walls. It is likely that authors who found no cyst walls were examining old lesions.
|
|
Subepidermal Calcified Nodule
In subepidermal calcified nodule, also referred to as cutaneous calculi, usually a single small, raised, hard nodule is present. Occasionally, however, there are two or three nodules , and in some instances, there are numerous or even innumerable nodules. Most patients are children; however, in some patients, a nodule is present at birth or
|
|
does not appear until adulthood . In most instances, the surface of the nodule is verrucous, but it may be smooth. The most common location of the nodule is the face.
|
Pathogenesis. The primary event seems to be the formation of large, homogeneous masses that undergo calcification and break up into numerous calcified globules . The origin of the homogeneous masses is obscure. It is not likely that they originate from a specific preexisting structure, such as sweat ducts or nevus cells as has been assumed
|
|
|
|