
👤 Users: 0 | 👁 Guests: 1 | 🌍 Total: 1
Acne keloidalis nuchae =العد الجدري




































Acne keloidalis nuchae
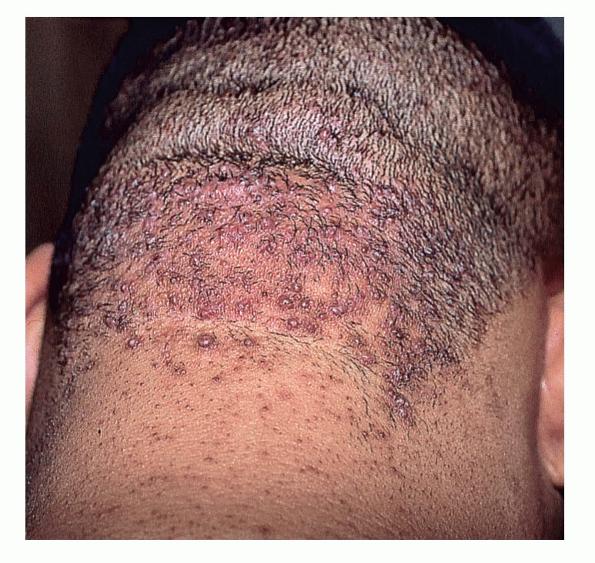
Acne keloidalis nuchae (AKN) is a scarring form of chronic folliculitis that manifests as follicular-based papules and pustules, which eventuates in keloidlike lesions. The lesions are most pronounced on the occipital scalp and the posterior part of the neck, and they occur almost exclusively in young males of African descent.1 The term acne keloidalis nuchae is somewhat of a misnomer because the lesions do not occur as a result of acne vulgaris and are histologically not keloidal.2
Acne keloidalis nuchae was first recognized as a discrete entity in the late 1800s. Hebra was the first to describe and document this condition in 1860, under the name sycosis framboesiformis. Subsequently in 1869, Kaposi described this same condition as dermatitis papillaris capillitii.3 The term acne keloidalis was then given to this condition in 1872 by Bazin, and, since that time, this is the name most often used in the literature.2
Clinically, the lesions initially manifest as mildly pruritic follicular-based papules and pustules on the nape of the neck. Because the folliculitis is persistent, ultimately keloidlike plaques eventuate. The area is typically hairless, but broken hair shafts, tufted hairs, and ingrown hairs can sometimes be identified within and at the margins of the plaques. Over time, the plaques typically slowly expand. The lesions are disfiguring and can be painful. Abscesses and sinus tracts with purulent discharge may develop in advanced cases. Comedones are not a common feature of acne keloidalis nuchae.
Pathophysiology
The exact etiology of acne keloidalis nuchae (AKN) remains obscure; however, one postulation is that chronic irritation and inward growth of coarse, curved hairs may play a role in the development of these lesions. This hypothesis is supported by the fact that lesions are exacerbated by close shaving and/or recurrent rubbing of the area by clothes or athletic gear. In a study of 453 high school, college, and professional American football players, 13.6% of African American athletes had acne keloidalis nuchae, whereas none of the white athletes had acne keloidalis nuchae.4
Similar to pseudofolliculitis barbae, a condition that also occurs more commonly in African Americans, some have proposed that close shaving or shearing of coarse, curved hairs facilitates the reentry of the free end of the hair into the skin, which then invokes an acute inflammatory response. Men who have haircuts more frequently than once a month are at higher risk of developing acne keloidalis nuchae.5
Although the ingrowing hairs account for small papules, they are not sufficient to explain the progressive scarring alopecia that occurs in some patients. Patients with progressive scarring alopecia often exhibit recurrent crops of small pustules and may have a condition akin to folliculitis decalvans. Chronic low-grade bacterial infection, autoimmunity, and some types of medication (eg, cyclosporine, diphenylhydantoin, carbamazepine) have also been implicated in the pathogenesis in some patients.6,7
Sperling et al classify acne keloidalis nuchae as a primary form of inflammatory scarring alopecia and suggest that overgrowth of microorganisms does not play an essential role in the pathogenesis of acne keloidalis nuchae. They also found no association between pseudofolliculitis barbae and acne keloidalis nuchae.8
After extensive histological and ultrastructural studies of acne keloidalis nuchae lesions, Herzberg et al proposed that a series of events must happen in order for acne keloidalis nuchae to occur, namely the following9 :
- The initial process begins as acute perifollicular inflammation followed by weakening of the follicular wall at the level of the lower infundibulum, the isthmus, or both.
- The naked hair shaft is then released into the surrounding dermis, which acts as a foreign body and incites further acute and chronic granulomatous inflammation. This process is clinically manifested by small follicular-based papules and pustules.
- Subsequently, fibroblasts deposit new collagen and fibrosis ensues.
- Distortion and occlusion of the follicular lumen by the fibrosis results in retention of the hair shaft in the inferior aspect of the follicle, thereby perpetuating the granulomatous inflammation and scarring. This stage is marked by plaques of hypertropic scar
History
Importantly, note the duration of acne keloidalis nuchae (AKN), the duration of the acute flare, past therapeutic successes and failures, present medications, hair grooming techniques, and any known allergies. Regardless of symptomology, in general the lesions are cosmetically bothersome.
Early papular lesions are usually asymptomatic, but pustular lesions are often pruritic and occasionally painful. Large lesions can be painful. Abscesses and sinuses may be present and may emit purulent, malodorous discharge. Hats, shirts, jackets, and sweaters can irritate the involved area.
Physical
Early lesions manifest as firm, dome-shaped, follicular-based papules that are 2-4 mm in diameter. The papules are predominately located on the occipital region and nape of the neck. Pustules may be present, but often only excoriated papules can be identified because the lesions are often pruritic or they become traumatized when the hair is groomed.
As the disease progresses, more papules and pustules appear and, over time, can coalesce to form larger plaques.
Causes
Suggested etiologies include the following:
- Close shaving of the neck: This often exacerbates the condition. The sharp, curved hairs reenter the skin and invoke an acute inflammatory response.
- Constant irritation from shirt collars or athletic gear: This irritation causes shearing of the hairs.
- Chronic low-grade bacterial infections
- An autoimmune process
- Use of antiepileptic drugs or cyclosporine
- An increased number of mast cells in the occipital region11
Reports have linked acne keloidalis nuchae with keratosis follicularis spinulosa decalvans, a rare X-linked disorder in which individuals have a genetic predisposition toward follicular hyperkeratosis and subsequent inflammation.12,13
Laboratory Studies
Bacterial culture and sensitivity testing of acne keloidalis nuchae (AKN) pustules and draining sinuses should be considered. If pathogenic microorganisms are identified, appropriate antibiotics should be prescribed.
Procedures
A biopsy may be performed if the clinical presentation is atypical and to exclude other similar conditions.
Histologic Findings
The histological findings vary depending on the timing of the biopsy. The initial infiltrate is primarily composed of neutrophils and lymphocytes that are distributed around the lower infundibulum and isthmus of the hair follicle. Subsequently, the follicle and sebaceous glands are destroyed, with liberation of the naked hair shafts into the dermis. Acute and granulomatous inflammation surrounds the free hair shafts, and, ultimately, fibrosis ensues. Scarring alopecia ensues in long-standing lesions, marked by dermal fibrosis associated with numerous plasma cells. True keloidal collagen is typically not a feature.
Often, acute and chronic inflammation may be present in the same region, because new lesions often develop adjacent to chronic lesions. Sinus tracks can be identified in long-standing lesions. Intact hair follicles at the margins may exhibit polytrichia, with more than one hair shaft noted in a single follicle, but this is physiologic for the occiput.14 Individual early papules may also demonstrate ingrown hairs, and these may be seen clinically in patients without progressive scarring alopecia
Treatment of acne keloidalis nuchae (AKN) is difficult, and numerous modalities have been used with varying degrees of success.
- Education is the key to prevention. Patients need to be made aware that the condition is not caused by unclean clippers but, rather, is exacerbated by short haircuts and close shaving. In addition, patients should be educated to avoid tight-fitting collared shirts and athletic head gear, which may lead to mechanical shearing of the hairs.
- Initiating therapy as quickly as possible after the initial appearance of lesions decreases the chance of long-term cosmetic disfigurement.15 Daily shampooing with gently foaming benzoyl peroxide washes, chlorhexidine, or mild keratolytic cleansers containing alpha-hydroxy acids or tar is an effective alternative to standard shampoo products. Discontinuance of hair greases and hair pomades should also be advised.16
- Early, mild papular disease may respond to potent or superpotent topical steroids with or without the use of topical retinoids. This latter combination seems to be somewhat more effective than class 1 or 2 steroids alone. One suggested regimen includes twice-a-day treatment with a combined retinoic acid (Retin-A) and a class 2 or 3 corticosteroid cream or gel.
- When pustules, crust, or drainage is present, use of a topical antibiotic such as clindamycin or erythromycin on a twice-daily basis until the pustules abate may be advantageous. If the patient does not have significant improvement in 4-5 days, a bacterial culture of the involved area should be performed, and, if pathogenic microorganisms are identified, appropriate systemic antibiotics should be initiated. These antibiotics are instituted for both their antibiotic and anti-inflammatory effects. Topical chloramphenicol has been effective and can be prepared by adding 500 mg to 30 g of fluocinonide cream.
- In the rare cases in which large abscesses or draining sinuses are present, a 7- to 10-day tapering course of oral prednisone may be considered in addition to the appropriate systemic antibiotics.
- Isotretinoin may be considered for rapidly progressive disease.
- Intralesional triamcinolone acetonide injection (3-5 mg/mL, up to 40 mg/mL for resistant lesions) of papular lesions is another option. Application of a lidocaine-prilocaine cream mixture under plastic film occlusion 2 hours prior to the injection decreases the pain of injections. Warn patients that the area injected might become hypopigmented and remain so for 6-12 months. Some authors advocate electrodesiccation or liquid nitrogen prior to injection to facilitate the process.16
- An adjunctive therapy to intralesional steroids is to shave or curette the small papules or nodules prior to injection.
- Intralesional 5-fluorouracil and/or immunotherapy sessions have also been used.
- Cryotherapy has also proven to be successful in some cases.17 The area is frozen for 20 seconds, allowed to thaw, and is then frozen again 1 minute later. The morbidity (discomfort and drainage) is greater than other modalities, and the treated site often becomes hypopigmented because of destruction of the melanocytes and may remain so for up to 12-18 months.
- Another option is radiation therapy, which causes permanent epilation of the area.
- Once healing has occurred and active disease is controlled, apply a tretinoin-fluorinated steroid mixture to the occipital part of the scalp twice daily to help prevent recurrence.
Surgical Care
- Laser ablation using various lasers (eg, carbon dioxide, 1064-nm Nd:YAG, 810-nm diode) should be considered for lesions refractory to other treatments.18 One case series showed that 4 monthly laser hair epilation sessions using the diode laser (810 nm) in addition to a topical retinoid and steroid resulted in long-lasting improvement in the appearance and prevention of lesions. Laser hair epilation allows for coagulation necrosis of both viable hair follicles and fragmented hair shafts in the deep dermis.19
- Excision of small papules via punch biopsy is another therapeutic option. The punch should extend deep into the subcutaneous tissue so that the entire hair follicle is excised. Superficial biopsies tend to have a much higher incidence of recurrence.
- After the punch biopsy is performed, the wound edges can be injected with 10-40 mg/mL of triamcinolone acetonide to reduce inflammation.
- The area should be reapproximated using 4-0 suture. Because nylon sutures often irritate the skin, silk sutures can be used to prevent this problem.
- Instruct patients to clean the postoperative area 3 times a day with a mild cleanser, followed by application of a topical antibiotic ointment.
- The sutures should be removed in 7-10 days, and the patient should then begin a twice-daily topical retinoic acid/corticosteroid regimen for 4-6 weeks.
- Injection of 3-5 mg/mL triamcinolone acetonide may also be considered if the area remains indurated. The postoperative surgical site can be injected every 2-4 weeks until the area softens.
- The preferred method of excision for larger linear lesions (1 cm or less in diameter) is a horizontal ellipse with primary closure; however, allowing the lesion to heal by secondary intention is a viable option for lesions that cannot be easily closed primarily.20 The excision should extend below the hair follicles, and the area should be reapproximated with 4-0 silk sutures.
- Always remember that when closing the area, ensure the patient’s neck is not in a flexed position; otherwise, the patient will spend a week or longer having to look upward.
- An important caveat with surgical excision is that primary closure often results in recurrences and/or hypertrophic scarring, and data show that allowing lesions to heal by secondary intention results in fewer recurrences. Wound healing is typically achieved within 6-10 weeks, and, in general, the surgical site contracts to an area smaller and flatter than the original site.21,22
- Postoperative care is basically the same as with punch grafts.
- Pain medication may be necessary for the first 48 hours.
- Have patients return in 24-36 hours (preferably with the person responsible for changing dressings) for removal of the initial dressing. Soak the area with sodium chloride solution to facilitate the removal of the dressing and to clean the postoperative site.
- Instruct patients to start cleaning the site twice a day (following the regimen above) once the dressing is removed.
- Instruct patients to return for follow-up in 1 week, or, sooner, if any complications occur.
- Instruct patients to return for follow-up care for possible initiation of intralesional steroid injections or to begin topical steroid/retinoic acid therapy once the area has healed, usually in 2-3 months. Do not begin intralesional steroids prior to complete would healing because this can result in wound dehiscence.
- A follicular papule or pustule occasionally develops along the border of the linear scar. Treat all inflammatory lesions with topical clindamycin or chloramphenicol until the infection subsides. The residual papule can then be treated with topical or intralesional steroids or excised via a punch biopsy.
- Excision followed by grafting is typically not cosmetically acceptable because it results in a large, depressed, non–hair-bearing area.
Medication
The goals of pharmacotherapy are to reduce inflammation and eliminate infection, if present.
Corticosteroids
These agents are used for their anti-inflammatory properties, but they must be used with caution because they have local and systemic side effects.
Topical corticosteroids may be used alone or in combination retinoic acid.
Triamcinolone (Kenalog, Amcort)
For inflammatory reactions responsive to steroids; decreases inflammation by suppressing migration of PMN leukocytes and reversing capillary permeability.
- Dosing
- Interactions
- Contraindications
- Precautions
Adult
Small papules: 3-5 mg/mL q2-4wk until lesions resolve or flatten
Larger keloidlike plaques or at margins of postoperative site: 10-40 mg/mL q2-4wk until lesions resolve or flatten
Pediatric
Not established
- Dosing
- Interactions
- Contraindications
- Precautions
Coadministration with barbiturates, phenytoin, and rifampin decreases effects
- Dosing
- Interactions
- Contraindications
- Precautions
Documented hypersensitivity; fungal, viral, and bacterial skin infections
- Dosing
- Interactions
- Contraindications
- Precautions
Pregnancy
C – Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Hypopigmentation, steroid atrophy, delayed wound healing, rare cases of adverse systemic effects
Prednisone (Deltasone, Meticorten, Orasone)
May decrease inflammation by reversing increased capillary permeability and suppressing PMN activity. Used when patient has acute flare.
- Dosing
- Interactions
- Contraindications
- Precautions
Adult
40-80 mg PO qam
Pediatric
Not established
- Dosing
- Interactions
- Contraindications
- Precautions
Coadministration with estrogens may decrease clearance; concurrent use with digoxin may cause digitalis toxicity secondary to hypokalemia; phenobarbital, phenytoin, and rifampin may increase metabolism of glucocorticoids (consider increasing maintenance dose); monitor for hypokalemia with coadministration of diuretics
- Dosing
- Interactions
- Contraindications
- Precautions
Documented hypersensitivity; viral, fungal, tubercular skin, or connective-tissue infections; peptic ulcer disease; hepatic dysfunction; GI disease
- Dosing
- Interactions
- Contraindications
- Precautions
Pregnancy
C – Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Increased infections, hyperglycemia, edema, osteonecrosis, peptic ulcer disease myopathy, peptic ulcer disease, hypokalemia, osteoporosis, euphoria, psychosis, myasthenia gravis, and growth suppression may occur; abrupt discontinuation of glucocorticoids may cause adrenal crisis
Clobetasol propionate (Olux)
Available as a 0.05% foam (Olux).
- Dosing
- Interactions
- Contraindications
- Precautions
Adult
Either used alone with twice-daily dosing or mix with equal parts of retinoic acid and apply sparingly to affected areas twice daily; do not use occlusive dressing
Pediatric
Not established
- Dosing
- Interactions
- Contraindications
- Precautions
None reported
- Dosing
- Interactions
- Contraindications
- Precautions
Documented hypersensitivity; fungal, viral, or tubercular skin lesions; herpes simplex or herpes zoster
- Dosing
- Interactions
- Contraindications
- Precautions
Pregnancy
C – Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Use over large or denuded areas of body for prolonged periods with an occlusive dressing or on infants may produce adverse systemic effects; complications may include steroid atrophy, steroid acne, delayed wound healing, and rare cases of adverse systemic effects if used over large areas and/or under occlusion
Fluocinonide (Lidex) or Mometasone furoate (Elocon)
Class 2 steroid (potent). Fluocinonide available as a 0.05% cream, ointment, and gel, and mometasone furoate available as 0.1% ointment.
- Dosing
- Interactions
- Contraindications
- Precautions
Adult
Use alone with twice-daily dosing or mix with equal parts retinoic acid and apply bid sparingly to affected areas; do not use occlusive dressing
Pediatric
Not established
- Dosing
- Interactions
- Contraindications
- Precautions
None reported
- Dosing
- Interactions
- Contraindications
- Precautions
Documented hypersensitivity; herpes simplex infection; fungal, viral, or tubercular skin lesions
- Dosing
- Interactions
- Contraindications
- Precautions
Pregnancy
C – Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Complications may include steroid atrophy, steroid acne, delayed wound healing, and rare cases of adverse systemic effects if used over large areas and/or under occlusion
Retinoids
Although the exact mechanism of action is unknown, retinoids decrease the cohesiveness of abnormal hyperproliferative keratinocytes, modulate keratinocyte differentiation, and have anti-inflammatory properties.
Isotretinoin (Accutane)
Oral agent that treats serious dermatologic conditions. Synthetic 13-cis isomer of the naturally occurring tretinoin (trans -retinoic acid). Both agents are structurally related to vitamin A.
Decreases sebaceous gland size and sebum production. May inhibit sebaceous gland differentiation and abnormal keratinization.
A US Food and Drug Administration–mandated registry is now in place for all individuals prescribing, dispensing, or taking isotretinoin. For more information on this registry, see iPLEDGE. This registry aims to further decrease the risk of pregnancy and other unwanted and potentially dangerous adverse effects during a course of isotretinoin therapy.
- Dosing
- Interactions
- Contraindications
- Precautions
Adult
0.5-1.5 mg/kg/d PO (usually 1 mg/kg/d)
Pediatric
Not established
- Dosing
- Interactions
- Contraindications
- Precautions
Toxicity may occur with vitamin A coadministration; pseudotumor cerebri or papilledema may occur when coadministered with tetracyclines; may reduce plasma levels of carbamazepine and contraceptive efficacy
- Dosing
- Interactions
- Contraindications
- Precautions
Documented hypersensitivity
- Dosing
- Interactions
- Contraindications
- Precautions
Pregnancy
X – Contraindicated; benefit does not outweigh risk
Precautions
May decrease night vision; inflammatory bowel disease may occur; may be associated with development of hepatitis; occasional exaggerated healing response of acne lesions (excessive granulation with crusting) may occur
Diabetes patients may experience problems controlling blood glucose while on isotretinoin; avoid exposure to UV light or sunlight until tolerance achieved; discontinue treatment if rectal bleeding, abdominal pain, or severe diarrhea occur
Mood swings or depression may occur; caution if history of depression
Tretinoin topical (Retin-A)
Although exact mechanism of action is unknown, retinoids decrease cohesiveness of abnormal hyperproliferative keratinocytes, modulate keratinocyte differentiation, and have anti-inflammatory properties.
Available as 0.025%, 0.05%, and 0.1% creams. Also available as 0.01% and 0.025% gels.
- Dosing
- Interactions
- Contraindications
- Precautions
Adult
Can be used alone or mix with equal parts class 2 or 3 corticosteroid cream or gel and apply bid
Pediatric
Not established
- Dosing
- Interactions
- Contraindications
- Precautions
Possible neutralization with simultaneous use of benzyl peroxide, and increased irritation with concomitant use of salicylic acid, resorcinol, topical sulfur, other keratolytics, abrasives, and astringents
- Dosing
- Interactions
- Contraindications
- Precautions
Documented hypersensitivity
- Dosing
- Interactions
- Contraindications
- Precautions
Pregnancy
C – Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Photosensitivity may occur with excessive sunlight exposure; caution in eczema; do not apply to mucous membranes, mouth, and angles of nose
Antibiotics
Empiric antimicrobial therapy must be comprehensive and should cover all likely pathogens in the context of this clinical setting.
Erythromycin base (E-Mycin, Erythrocin)
Inhibits bacterial growth, possibly by blocking dissociation of peptidyl t-RNA from ribosomes, causing RNA-dependent protein synthesis to arrest. For treatment of staphylococcal and streptococcal infections. Age, weight, and severity of infection determine proper dosage in children. When twice-daily dosing is desired, half total daily dose may be taken q12h. Double the dose for more severe infections.
- Dosing
- Interactions
- Contraindications
- Precautions
Adult
250 mg PO qid
Pediatric
Not established
- Dosing
- Interactions
- Contraindications
- Precautions
Coadministration may increase toxicity of theophylline, digoxin, carbamazepine, and cyclosporine; may potentiate anticoagulant effects of warfarin; coadministration with lovastatin and simvastatin increases risk of rhabdomyolysis
- Dosing
- Interactions
- Contraindications
- Precautions
Documented hypersensitivity; hepatic impairment
- Dosing
- Interactions
- Contraindications
- Precautions
Pregnancy
B – Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions
Caution in liver disease; estolate formulation may cause cholestatic jaundice; adverse GI effects are common (give doses pc); discontinue use if nausea, vomiting, malaise, abdominal colic, or fever occur
Mupirocin (Bactroban)
Topical antibiotic; inhibits bacterial growth by inhibiting RNA and protein synthesis.
- Dosing
- Interactions
- Contraindications
- Precautions
Adult
Apply topically bid
Pediatric
Apply as in adults
- Dosing
- Interactions
- Contraindications
- Precautions
None reported
- Dosing
- Interactions
- Contraindications
- Precautions
Documented hypersensitivity
- Dosing
- Interactions
- Contraindications
- Precautions
Pregnancy
B – Fetal risk not confirmed in studies in humans but has been shown in some studies in animals
Precautions
Prolonged use may result in growth of nonsusceptible organisms
Doxycycline (Vibramycin)
Broad-spectrum, synthetically derived bacteriostatic antibiotic in the tetracycline class. Almost completely absorbed, concentrates in bile, and is excreted in urine and feces as a biologically active metabolite in high concentrations.
Inhibits protein synthesis and, thus, bacterial growth by binding to 30S and possibly 50S ribosomal subunits of susceptible bacteria. May block dissociation of peptidyl t-RNA from ribosomes, causing RNA-dependent protein synthesis to arrest.
- Dosing
- Interactions
- Contraindications
- Precautions
Adult
200 mg PO/IV immediately and 100 mg hs, followed by 100 mg bid; alternatively, 100-200 mg PO bid
Pediatric
<8 years: Not recommended
>8 years: 2-5 mg/kg/d PO/IV in 1-2 divided doses; not to exceed 200 mg/d
- Dosing
- Interactions
- Contraindications
- Precautions
Bioavailability decreases with antacids containing aluminum, calcium, magnesium, iron, or bismuth subsalicylate; can increase hypoprothrombinemic effects of anticoagulants; can decrease effects of oral contraceptives, causing breakthrough bleeding and increased risk of pregnancy
- Dosing
- Interactions
- Contraindications
- Precautions
Documented hypersensitivity; severe hepatic dysfunction
- Dosing
- Interactions
- Contraindications
- Precautions
Pregnancy
D – Fetal risk shown in humans; use only if benefits outweigh risk to fetus
Precautions
Photosensitivity may occur with prolonged exposure to sunlight or tanning equipment; reduce dose in renal impairment; consider drug serum level determinations in prolonged therapy; tetracycline use during tooth development (last half of pregnancy through age 8 y) can cause permanent discoloration of teeth; Fanconilike syndrome may occur with outdated tetracyclines
Rifampin (Rifadin, Rimactane)
Inhibits RNA synthesis in bacteria by binding to beta-subunit of DNA-dependent RNA polymerase, which, in turn, blocks RNA transcription.
- Dosing
- Interactions
- Contraindications
- Precautions
Adult
10 mg/kg/d mg PO/IV qd; not to exceed 600 mg/d
Pediatric
10-20 mg/kg PO/IV; not to exceed 600 mg/d