Tinea corporis refers to all dermatophytoses of glabrous skin except the palms, soles, and groin.
EPIDEMIOLOGY
Tinea corporis may be transmitted directly from infected humans or animals, via fomites, or via autoinoculation from reservoirs such as T. rubrum colonization of the feet. Children are more likely to contract zoophilic pathogens, especially M. canis from dogs or cats. Occlusive clothing and a warm, humid climate are associated with more frequent and severe eruptions.
The occlusive clothing, frequent skin-to-skin contact, and minor trauma (mat burns) of competitive wrestling create an environment in which dermatophytes flourish. Numerous outbreaks of “tinea corporis gladiatorum” have resulted, mostly caused by T. tonsurans.
Variants of Tinea Capitis
NAME
ETIOLOGY
CLINICAL DESCRIPTION
Noninflammatory
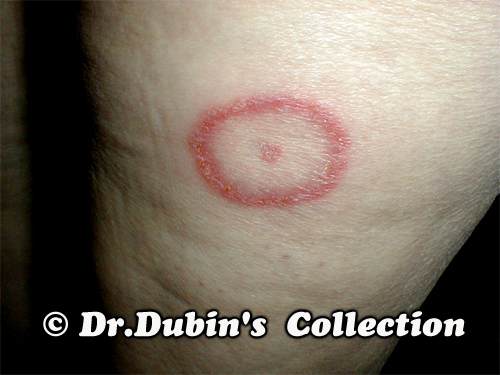
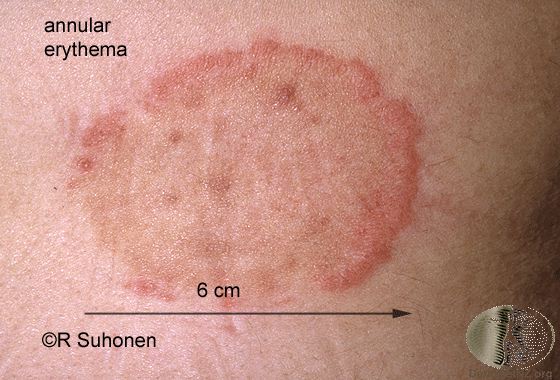
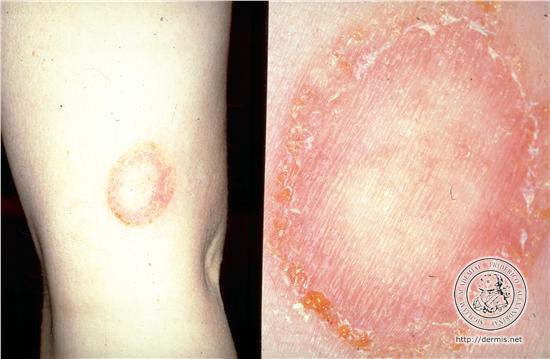
Tinea circinata
Any dermatophyte (usually Trichophyton rubrum, T. mentagrophytes, Microsporum canis)
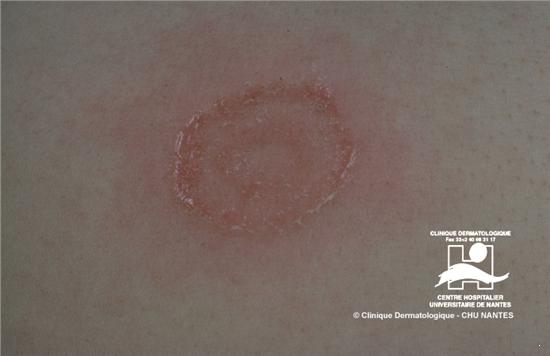
Annular lesions with central clearing and an active, spreading border
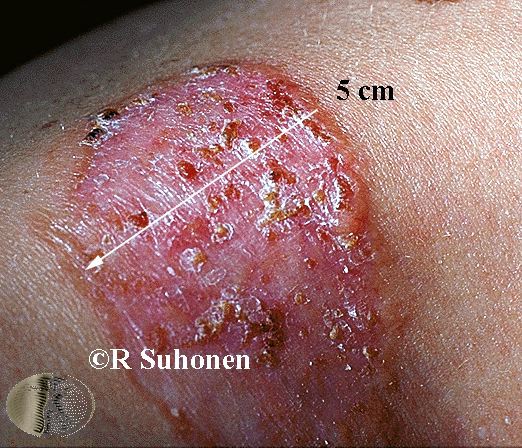
Bullous tinea corporis
Usually T. rubrum
Spongiotic or sub-corneal vesicles/pustules; may be herpetiform
Tinea imbricata
T. concentricum
Widespread; multiple concentric, polycyclic scaly lesions with minimal inflammation
Inflammatory
Kerion of glabrous skin
Zoophilic organisms
Similar to kerion of scalp or beard
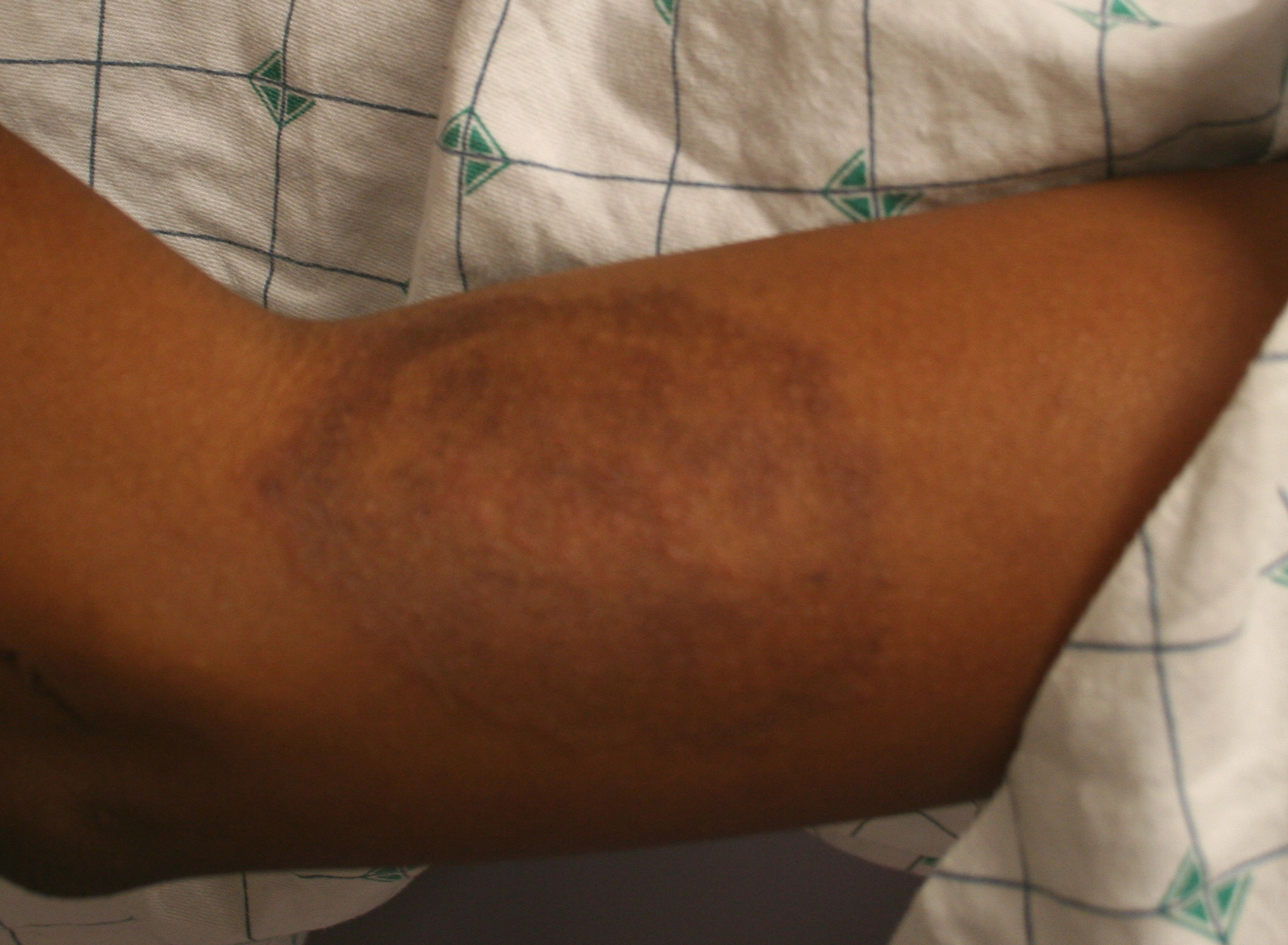
Majocchi granuloma
T. rubrum, T. violaceum, T. tonsurans, T. mentagrophytes
Perifollicular, granulomatous nodules mostly on the scalps of children; often without pustulation, and associated with underlying disease
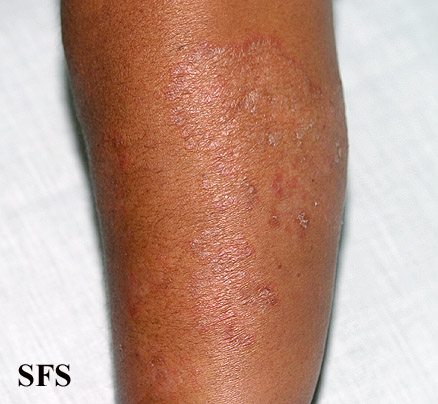
Nodular granulomatous perifolliculitis of the legs
T. rubrum
Variant of Majocchi granuloma affecting the lower two-thirds of women's legs; unilateral; T. rubrum is also present on the nails and feet
Agminate folliculitis
Zoophilic organisms
Well-defined erythematous plaques studded with perifollicular pustules
Subcutaneous abscess (tinea profunda)
T. mentagrophytes, T. violaceum, T. tonsurans, T. rubrum, M. audouinii
Deep subcutaneous nodules are present; rarely with lymph node involvement or hematogenous spread
Mycetoma
M. audouinii, M. canis, M. ferrugineum, T. mentagrophytes, T. tonsurans, T. violaceum, T. verrucosum
Subcutaneous masses
Tinea faciale
Usually Trichophyton species, occasionally M. canis
3%-4% of tinea corporis, erythematous, scaly plaques with or without active borders; telangiectasia, atrophy, and photo-exacerbation may mimic lupus erythematosus
Tinea incognito
Any dermatophyte infection modified by glucocorticoids
Atypical with possible absence of inflammation, scaling, or symptoms; dermal nodules or kerion-like lesions may be present
Tinea imbricata, caused by T. concentricum, clinically appears as a plaque consisting of concentric erythematous rings. It is largely limited to areas of the Far East, South Pacific, and South and Central America.
ETIOLOGY
Although any dermatophyte can cause tinea corporis, the most common cause is T. rubrum. T. mentagrophytes, M. canis, and T. tonsurans are also common pathogens.3 T. rubrum and T. verrucosum are the most likely candidates in cases with additional follicular involvement.28 Tinea imbricata is caused by T. concentricum.
CLINICAL FINDINGS
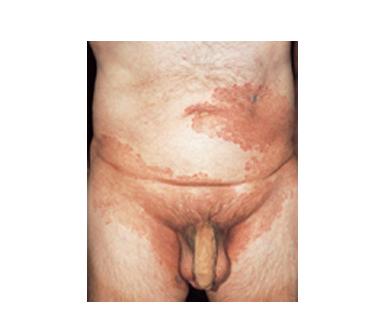
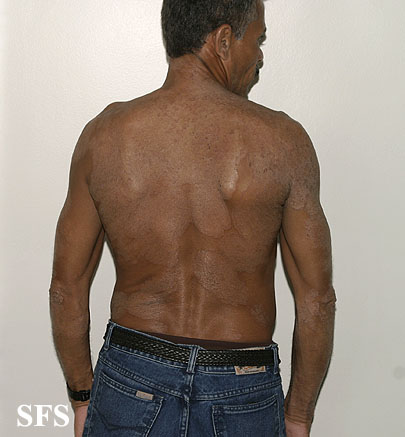
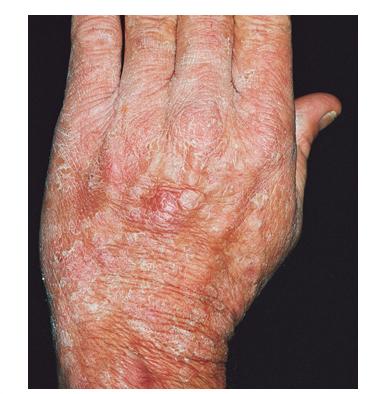
The classic presentation is an annular lesion with scale across the entire erythematous border. The border is often vesicular and advances centrifugally. The center of the lesion is usually scaly but may exhibit clearing. Lesions may be serpiginous and annular . Concentric vesicular rings suggest tinea incognito caused by T. rubrum, whereas the concentric rings of tinea imbricata demonstrate little to no vesiculation. T. rubrum infections may also present as large,
confluent polycyclic or psoriasiform plaques .
Majocchi granuloma is an infection usually caused by T. rubrum, which occurs when fungal hyphae invade hairs and hair follicles. It is classically seen in women who shave their legs and appears as inflamed folliculocentric papules.