
Contact Us :
👤 Users: 0 | 👁 Guests: 3 | 🌍 Total: 3
Erythroderma = الاحمرية الجلدية










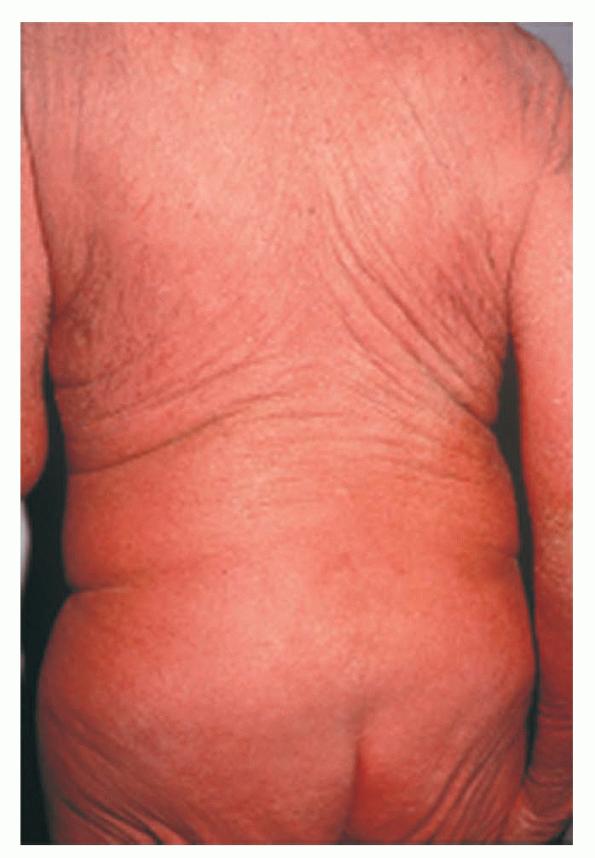













Erythroderma
Exfoliative dermatitis (ED) is a definitive term that refers to a scaling erythematous dermatitis involving 90% or more of the cutaneous surface. Exfoliative dermatitis is characterized by erythema and scaling involving the skin’s surface and often obscures the primary lesions that are important clues to understanding the evolution of the disease. Clinicians are challenged to find the cause of exfoliative dermatitis by eliciting the history of illness prior to erythema and scaling, by probing with biopsies, and by performing blood studies.
The term red man syndrome is reserved for idiopathic exfoliative dermatitis in which no primary cause can be found, despite serial examinations and tests. Idiopathic exfoliative dermatitis is characterized by marked palmoplantar keratoderma, dermatopathic lymphadenopathy, and a raised level of serum immunoglobulin E (IgE) and is more likely to persist than other types.
The term l’homme rouge refers to exfoliative dermatitis that is secondary to cutaneous T-cell lymphoma. The historic classification of exfoliative dermatitis into Wilson-Brocq (chronic process associated with exacerbation and remissions), Hebra or pityriasis rubra (relentlessly progressive disease), and Savill (self-limiting) types lacks any clinical significance.
Pathophysiology
An increased skin blood perfusion occurs in exfoliative dermatitis that results in temperature dysregulation (resulting in heat loss and hypothermia) and possible high-output cardiac failure. The basal metabolic rate rises to compensate for the resultant heat loss. Fluid loss by transpiration is increased in proportion to the basal metabolic rate. The situation is similar to that observed in patients following burns (negative nitrogen balance characterized by edema, hypoalbuminemia, loss of muscle mass).
A marked loss of exfoliated scales occurs that may reach 20-30 g/d. This contributes to the hypoalbuminemia commonly observed in exfoliative dermatitis. Hypoalbuminemia results, in part, from decreased synthesis or increased metabolism of albumin. Edema is a frequent finding, probably resulting from fluid shift into the extracellular spaces. Immune responses may be altered, as evidenced by increased gamma-globulins, increased serum IgE in some cases, and CD4+ T-cell lymphocytopenia in the absence of HIV infection.
History
History is the most important aid in diagnosing exfoliative dermatitis (ED).
- Patients may have a history of the primary disease (eg, psoriasis, atopic dermatitis).
- Elicit a comprehensive drug history, including over-the-counter drugs.
- Disease usually evolves rapidly when it results from drug allergens, lymphoma, leukemia, or staphylococcal scalded skin syndrome.
- Disease evolution is more gradual when it results from psoriasis, atopic dermatitis, or the spread of primary disease.
- Pruritus is a prominent and frequent symptom.
- Malaise, fever, and chills may occur.
Physical
- Patients often present with generalized erythema.
- Scaling appears 2-6 days after the onset of erythema, usually starting from flexural areas.
- Pruritus commonly results in excoriations.
- When exfoliative dermatitis persists for weeks, hair may shed; nails may become ridged and thickened and also may shed.
- Periorbital skin may be inflamed and edematous, resulting in ectropion (with consequent epiphora).
- In chronic cases, pigmentary disturbances can occur (especially in darker-skinned races); patchy or widespread loss of pigment (resembling vitiligo) has been reported.
- Diligent search for residual signs of underlying disease occasionally yields dividends. Residual signs may include the following:
- Islands of sparing in pityriasis rubra pilaris
- Few typical psoriatic plaques in psoriasis
- Papules or oral lesions of lichen planus
- Superficial blisters of pemphigus foliaceus
- Erythematous papular lesions of an early drug eruption
- Dermatopathic lymphadenopathy can occur in exfoliative dermatitis not caused by lymphoma or leukemia. A lymph node biopsy is advised when lymph nodes exhibit lymphomatous characteristics (eg, large size, rubbery consistency) and the cause of exfoliative dermatitis is undetermined.
- The general picture is modified according to the nature of the underlying disease and the patient’s general physical condition.
Causes
Determining specific etiologies in exfoliative dermatitis often is not possible; however, it is necessary to attempt since etiology may impact disease course and management options. The list of conditions that can cause exfoliative dermatitis is extensive and continues to expand. Cutaneous diseases that cause exfoliative dermatitis and the systemic diseases associated with them include the following:
- Atopic dermatitis – Acute and chronic leukemia
- Contact dermatitis – Reticulum cell sarcoma
- Dermatophytosis – Carcinoma of rectum
- Hailey-Hailey disease – Carcinoma of fallopian tubes
- Leiner disease -Graft versus host disease
- Lichen planus – HIV infection
- Lupus erythematosus – Lymphoma (including Hodgkin disease)
- Mycosis fungoides -Multiple myeloma
- Pemphigoid – Carcinoma of lung
- Pemphigus foliaceus – Mycosis fungoides
- Pityriasis rubra pilaris – Reiter syndrome
- Psoriasis
- Sarcoid
- Seborrheic dermatitis
- Stasis dermatitis
The most common causes of exfoliative dermatitis are best remembered by the mnemonic device ID-SCALP. The causes and their frequencies are as follows:
- Idiopathic – 30%
- Drug allergy – 28%
- Seborrheic dermatitis – 2%
- Contact dermatitis – 3%
- Atopic dermatitis – 10%
- Lymphoma and leukemia – 14%
- Psoriasis – 8%
More than 60 drugs have been implicated in the causation of exfoliative dermatitis (see Table). In many cases of protracted exfoliative dermatitis classified as being of undetermined cause, careful follow-up care and reevaluation implicated atopic dermatitis in older patients, intake of drugs overlooked by the patient, and prelymphomatous eruption as causative factors.
Drugs Implicated in the Causation of Exfoliative Dermatitis
Table
| ACE inhibitors | Allopurinol | Aminoglutethimide | Amiodarone | Amitriptyline |
| Amoxicillin | Ampicillin | Arsenic | Aspirin | Atropine |
| Auranofin | Aurothioglucose | Barbiturates | Benactyzine | Beta-blockers |
| Beta carotene | Bumetanide | Bupropion | Butabarbital | Butalbital |
| Captopril | Carbamazepine | Carbidopa | Chloroquine | Chlorpromazine |
| Chlorpropamide | Cimetidine | Ciprofloxacin | Clofazimine | Clofibrate |
| Co-trimoxazole | Cromolyn | Cytarabine | Dapsone | Demeclocycline |
| Desipramine | Diazepam | Diclofenac | Diflunisal | Diltiazem |
Doxorubicin | Doxycycline | Enalapril | Etodolac | Fenoprofen |
Fluconazole | Fluphenazine | Flurbiprofen | Furosemide | Gemfibrozil |
Gold | Griseofulvin | Hydroxychloroquine | Imipramine | Indomethacin |
Isoniazid | Isosorbide | Ketoconazole | Ketoprofen | Ketorolac |
Lithium | Meclofenamate | Mefenamic Acid | Meprobamate | Methylphenidate |
Minocycline | Nalidixic Acid | Naproxen | Nifedipine | Nitrofurantoin |
Nitroglycerin | Nizatidine | Norfloxacin | Omeprazole | Penicillamine |
Penicillin | Pentobarbital | Perphenazine | Phenobarbital | Phenothiazines |
Phenylbutazone | Phenytoin | Piroxicam | Primidone | Prochlorperazine |
Propranolol | Pyrazolones | Quinapril | Quinidine | Quinine |
Retinoids | Rifampin | Streptomycin | Sulfadoxine | Sulfamethoxazole |
Sulfasalazine | Sulfisoxazole | Sulfonamides | Sulfonylureas | Sulindac |
Tetracycline | Tobramycin | Trazodone | Trifluoperazine | Trimethoprim |
| Vancomycin | Verapamil |
| ACE inhibitors | Allopurinol | Aminoglutethimide | Amiodarone | Amitriptyline |
| Amoxicillin | Ampicillin | Arsenic | Aspirin | Atropine |
| Auranofin | Aurothioglucose | Barbiturates | Benactyzine | Beta-blockers |
| Beta carotene | Bumetanide | Bupropion | Butabarbital | Butalbital |
| Captopril | Carbamazepine | Carbidopa | Chloroquine | Chlorpromazine |
| Chlorpropamide | Cimetidine | Ciprofloxacin | Clofazimine | Clofibrate |
| Co-trimoxazole | Cromolyn | Cytarabine | Dapsone | Demeclocycline |
| Desipramine | Diazepam | Diclofenac | Diflunisal | Diltiazem |
Doxorubicin | Doxycycline | Enalapril | Etodolac | Fenoprofen |
Fluconazole | Fluphenazine | Flurbiprofen | Furosemide | Gemfibrozil |
Gold | Griseofulvin | Hydroxychloroquine | Imipramine | Indomethacin |
Isoniazid | Isosorbide | Ketoconazole | Ketoprofen | Ketorolac |
Lithium | Meclofenamate | Mefenamic Acid | Meprobamate | Methylphenidate |
Minocycline | Nalidixic Acid | Naproxen | Nifedipine | Nitrofurantoin |
Nitroglycerin | Nizatidine | Norfloxacin | Omeprazole | Penicillamine |
Penicillin | Pentobarbital | Perphenazine | Phenobarbital | Phenothiazines |
Phenylbutazone | Phenytoin | Piroxicam | Primidone | Prochlorperazine |
Propranolol | Pyrazolones | Quinapril | Quinidine | Quinine |
Retinoids | Rifampin | Streptomycin | Sulfadoxine | Sulfamethoxazole |
Sulfasalazine | Sulfisoxazole | Sulfonamides | Sulfonylureas | Sulindac |
Tetracycline | Tobramycin | Trazodone | Trifluoperazine | Trimethoprim |
| Vancomycin | Verapamil |
Laboratory Studies
- Increased erythrocyte sedimentation rate, anemia, hypoalbuminemia, and hyperglobulinemia are frequent findings.
- Byer and Bachur2 report that the levels of glucose, calcium, and creatinine and the platelet and polymorphonuclear leukocyte counts are of prognostic significance in children who present with erythroderma and fever.
- Increased IgE may be observed in exfoliative dermatitis (ED) when caused by atopic dermatitis.
- Peripheral blood smears and bone marrow examination may be useful in a leukemia workup.
- Immunophenotyping, flow cytometry, and particularly, B- and T-cell gene rearrangement analysis may be helpful in confirming the diagnosis if lymphoma is strongly suspected.
- Skin scrapings may reveal hyphae or scabies mites.
- Cultures may show bacterial overgrowth or the herpes simplex virus.
- Perform HIV testing in the right setting; use polymerase chain reaction for viral detection, rather than enzyme-linked immunoassay, since exfoliative dermatitis has been reported to predict seroconversion in HIV infection.
- In a report by Griffiths et al,3 decreased CD4+ T-cell count was observed in patients with exfoliative dermatitis in the absence of HIV disease.
Imaging Studies
- Pursue further tests (eg, computed tomography scanning, magnetic resonance imaging, chest radiography, mammography) if the clinical features so indicate.
Other Tests
- If the cause of exfoliative dermatitis is in doubt, survey patients for occult tumors or cancers. Perform chest radiography and routine cancer screenings appropriate for age and sex (eg, mammogram, stool occult blood test, sigmoidoscopy, prostate examination, serum prostate specific antigen level, cervical smear).
- Patch testing can be performed to unveil contact allergens but should be performed only during periods of remission. In the patch test, include systemic drugs the patient was taking prior to the onset of exfoliative dermatitis.
- Direct immunofluorescence studies diagnosed at least 2 reported cases of pemphigoid erythroderma, according to Scrivener et al.4
Procedures
- Skin biopsies reveal nonspecific findings of spongiotic dermatitis; however, primary disease may be evident.
Histologic Findings
The appearance of exfoliative dermatitis usually masks the underlying disease’s specific histologic features. The most common histopathologic appearance is of either subacute or chronic dermatitis; however, biopsy is indicated, since diagnostic findings are present in 40% of cases. A search for the underlying cause is necessary because of possible prognostic and therapeutic implications. Detailed histopathologic analysis with clinicopathologic correlation is mandatory in the remaining cases for which a specific cause is not apparent. Often, repeated biopsies and hematologic studies may be necessary to detect specific conditions (eg, cutaneous T-cell lymphoma). Repeated biopsies have been reported to result in a diagnosis in 50% of cases that do not reveal specific findings initially.
Medical Care
Patients presenting acutely with exfoliative dermatitis (ED) often require admission for inpatient management because their total body functions (including intake and output) can require monitoring. Hospital admission should be seriously considered in pediatric patients who present with erythroderma and fever because this presentation is a predictor of hypotension and even toxic shock syndrome. The principle of management is to maintain skin moisture, avoid scratching, avoid precipitating factors, apply topical steroids, and treat the underlying cause and complications. exfoliative dermatitis commonly resists therapy until the underlying disease is treated (eg, phototherapy, systemic medications in psoriasis). Outcome is unpredictable in idiopathic exfoliative dermatitis. The course is marked by multiple exacerbations, and prolonged glucocorticoid therapy often is needed.
- Discontinue all unnecessary medications. Carefully monitor and control fluid intake, since patients can dehydrate or go into cardiac failure; monitor body temperature, since patients may become hypothermic.
- Apply tap water–wet dressings (made from heavy mesh gauze); change every 2-3 hours. Apply intermediate-strength topical steroids (eg, triamcinolone cream 0.025-0.5%) beneath wet dressings. Suggest a tepid bath (may be comforting) once or more daily between dressing changes. Reduce frequency of dressings and gradually introduce emollients between dressing applications as exfoliative dermatitis improves.
- Institute systemic antibiotics if signs of secondary infection are observed. Antihistamines help reduce pruritus and provide needed sedation.
- Systemic steroids may be helpful in some cases but should be avoided in suspected cases of psoriasis and staphylococcal scalded skin syndrome.
- Increased capillary permeability occasionally is severe enough to justify plasma infusion.
- Preexisting malnutrition may become more marked and require nutritional intervention in older patients.
Consultations
Consult a dermatologist for all cases of exfoliative dermatitis.
Diet
Ensure adequate nutrition with emphasis on protein intake, since exfoliative dermatitis patients lose a lot of protein through excessive desquamation and show a tendency toward hypoalbuminemia. Alter diet as necessary if ingestion of a certain food group is suspected as the etiology of exfoliative dermatitis.
Activity
As tolerated
Medication
Topical steroids are the primary category of medications used to treat exfoliative dermatitis (ED). A sedative antihistamine may be a useful adjunct for pruritic patients, since it helps patients to sleep at night, thus limiting nocturnal scratching and excoriations. Antimicrobial agents often are used if an infection is suspected to be precipitating or complicating exfoliative dermatitis. Other drugs specifically indicated for management of underlying etiology of exfoliative dermatitis may be necessary.
Topical steroids
Exert anti-inflammatory effects by inhibiting early processes (eg, edema, fibrin deposition, capillary dilatation, movement of phagocytes into the area, phagocytic activities). In exfoliative dermatitis, they may inhibit the increased epidermal cell turnover that occurs. Indications include symptomatic relief of inflammation and/or pruritus associated with acute and chronic corticosteroid-responsive disorders.
Triamcinolone topical (Aristocort)
Medium-potency topical steroid. Use creams and lotions for moist weepy lesions and with intense inflammation (eg, exfoliative dermatitis). Frequency of use in exfoliative dermatitis depends on acute nature of disease and frequency with which wet dressings are changed.
Adult
Apply cream 0.025%, 0.1%, or 0.5% bid/qid
Apply lotion 0.025% or 0.1% bid/qid
Apply ointment 0.1% bid
Pediatric
Apply cream 0.025% qd/bid; 0.1% or 0.5% qd
Apply lotion 0.025% qd/bid; 0.1% qd
Apply ointment 0.1% qd/bid
None reported
Documented hypersensitivity; infections at treatment site or pre-existing skin atrophy
Pregnancy
C – Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Adrenal suppression, Cushing syndrome, intracranial hypertension, and growth retardation may occur as a result of systemic absorption of topical corticosteroids; children are more susceptible
Antihistamines
Exert both antipruritic and sedating effects. Used in treating histamine-mediated allergic reactions by competitively inhibiting H1 receptors on effector cells. To varying degrees, they exert sedative effects by crossing the blood-brain barrier and blocking central histaminogenic receptors.
Hydroxyzine (Atarax, Vistaril)
Antagonizes H1 receptors in periphery. May suppress histamine activity in subcortical region of CNS providing antipruritic effects
Adult
25-50 mg PO q4-6h prn
Pediatric
2-3 mg/kg/d PO divided tid/qid prn for pruritus (10 mg/5 mL syr)
May augment sedating effects of alcohol and other CNS depressants; may augment anticholinergic effects of anticholinergic drugs and drugs with anticholinergic effects
Documented hypersensitivity
Pregnancy
C – Fetal risk revealed in studies in animals but not established or not studied in humans; may use if benefits outweigh risk to fetus
Precautions
Avoid in hepatic impairment except in exceptional conditions; ECG abnormalities may occur (eg, alteration of T waves); warn patients of expected increase in drowsiness and to avoid tasks requiring alertness or physical dexterity; may exacerbate crises in porphyric patients