
Contact Us :
👤 Users: 0 | 👁 Guests: 3 | 🌍 Total: 3
Dyshidrotic eczema = اكزيمة عسر التعرق

























Dyshidrotic eczema
Dyshidrotic eczema is a recurrent or chronic relapsing form of vesicular palmoplantar dermatitis of unknown etiology. Dyshidrotic eczema also is termed pompholyx, which derives from cheiropompholyx, which means “hand and bubble” in Greek.
The etiology of dyshidrotic eczema is unresolved and is believed to be multifactorial. Dyshidrotic eczema is considered a reaction pattern caused by various endogenous conditions and exogenous factors.
Pathophysiology
The hypothesis of sweat gland dysfunction has been disputed because vesicular lesions have not been shown to be associated with sweat ducts. A 2009 case report provided clear histopathologic evidence that sweat glands do not play a role in dyshidrosis.1 However, hyperhidrosis is an aggravating factor in 40% of patients with dyshidrotic eczema. Improvement in pruritus, erythema, vesicles, and hand dermatitis with fewer or no signs of relapse has been obtained after botulinum toxin A injection.2
Dyshidrotic eczema may be associated with atopy and familial atopy. Of patients with dyshidrosis, 50% have atopic dermatitis.
Exogenous factors (eg, contact dermatitis to nickel, balsam, cobalt; sensitivity to ingested metals; dermatophyte infection; bacterial infection) may trigger episodes. These antigens may act as haptens with a specific affinity for palmoplantar proteins of the stratum lucidum of the epidermis. The binding of these haptens to tissue receptor sites may initiate pompholyx.
Evidence shows that the ingestion of metal ions such as cobalt can induce both type I and type IV hypersensitivity reactions, and, in addition, they can also act as atypical haptens activating T lymphocytes through human leucocyte antigen–independent pathways, causing systemic allergic dermatitis in the form of dyshidrotic eczema.3,4
Emotional stress5 and environmental factors (eg, seasonal changes, hot or cold temperatures, humidity) reportedly exacerbate dyshidrosis.
Dyshidrosis-like eczematous eruptions with the use of intravenous immunoglobulin infusions have been reported.
In some patients, a distant fungal infection can cause palmar pompholyx as an id reaction. In one study, one third of pompholyx occurrences on the palms resolved after treatment for tinea pedis.
Patients report pruritus of hands and feet with a sudden onset of vesicles. Burning pain or pruritus occasionally may be experienced before vesicles appear. Dyshidrotic eczema episodes vary in frequency from once per month to once per year. Patients with dyshidrotic eczema may report a variety of factors that possibly are related to eruptions, as follows:
- Emotional stress
- Personal or familial atopic diathesis (eg, asthma, hay fever, sinusitis)
- Certain work exposures (eg, cobalt) and/or recreational exposures
- Recent exposure to contact allergens (eg, nickel, balsams, paraphenylenediamine, chromate, sesquiterpene lactones) before condition flares
- Exposure to contact irritants before condition flares
- Recent exposure to costume jewelry (patients with palmar pompholyx and allergic to nickel)
- Recent treatment with intravenous immunoglobulin therapy8,9
- HIV related: Two cases were reported of HIV-positive patients who developed dyshidrotic eczema as an immune reconstitution inflammatory syndrome shortly after highly active antiretroviral therapy.10 Pompholyx has also been described as a manifestation of symptomatic HIV infection, including individuals who do not respond to topical and systemic therapies and whose condition resolves only after initiation of combination antiretroviral therapy.11
Physical
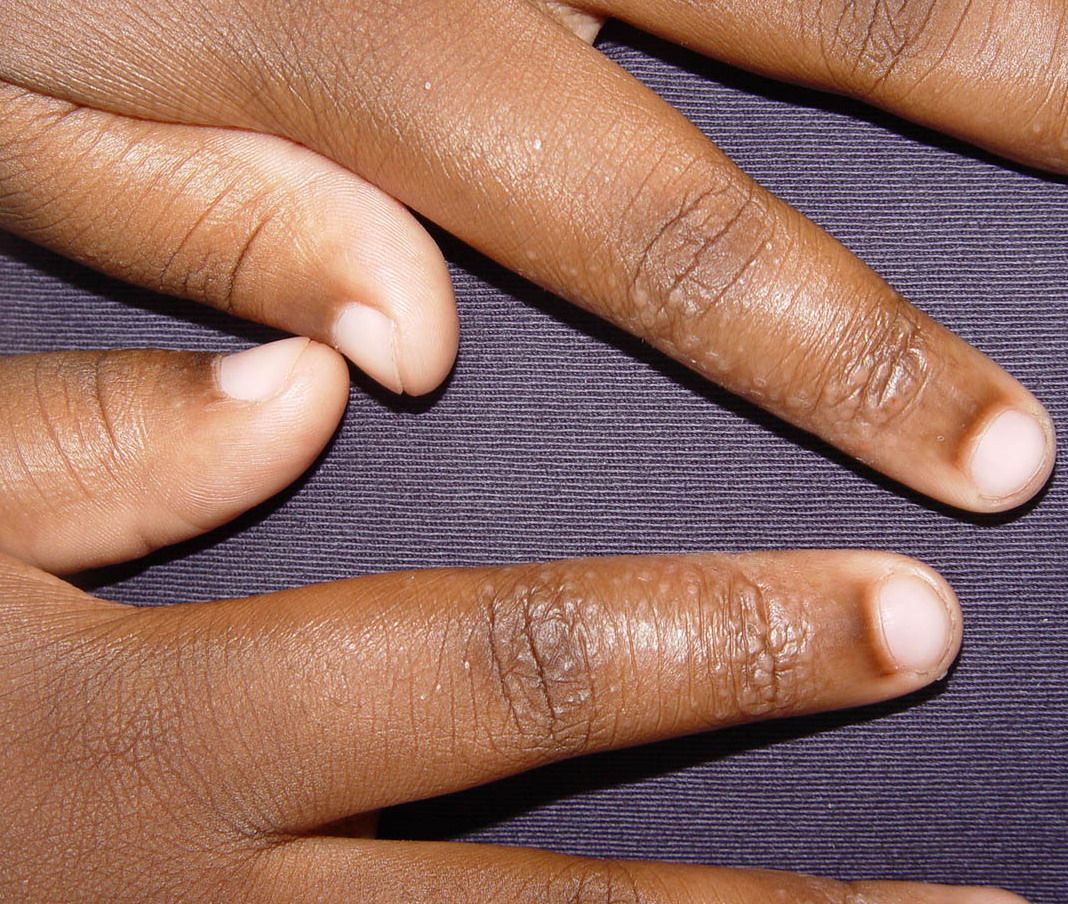
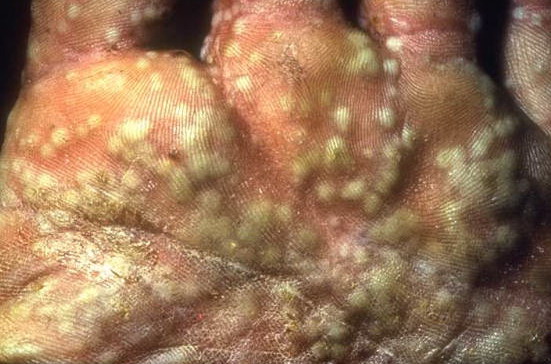
Symmetric crops of clear vesicles and/or bullae on the palms and lateral aspects of fingers characterize dyshidrotic eczema (see the images below). Feet, soles, and the lateral aspects of toes also may be affected
With long-standing disease, patients’ fingernails may reveal dystrophic changes (eg, irregular transverse ridging, pitting, thickening, discoloration). Interdigital maceration and desquamation of the interdigital spaces often are present, despite the possible absence of a dermatophyte infection. Vesicles and/or bullae may become infected secondarily, and pustular lesions may be present. Cellulitis and lymphangitis may develop.
The Dyshidrotic Eczema Area and Severity Index was developed based on severity grades for the number of vesicles per square centimeter, erythema, desquamation, itch, and the extent of affected areas.12 The index was found to be a simple standardized method for assessing the condition and was used to assess disease severity and treatment effectiveness in 2 clinical studies. Further evaluation with larger patient groups is needed
Causes
The cause of dyshidrotic eczema is unknown. The condition often appears related to other skin diseases (eg, atopic dermatitis, contact dermatitis, allergy to ingested metals, dermatophyte infection, bacterial infection, environmental or emotional stress). Several factors may participate in causing dyshidrotic eczema, as follows:
- Genetic factors: Monozygotic twins have been affected simultaneously by dyshidrotic eczema. The pompholyx gene has been mapped to band 18q22.1-18q22.3, in the autosomal dominant form of familial pompholyx.13
- Atopy: As many as 50% of patients with dyshidrotic eczema have reportedly had personal or familial atopic diathesis (eczema, asthma, hayfever, allergic sinusitis). The serum immunoglobulin E (IgE) level frequently is increased, even in patients who do not report a personal or familial history of atopy. Occasionally, dyshidrotic eczema is the first manifestation of an atopic diathesis.
- Nickel sensitivity: This may be a significant factor in dyshidrotic eczema. Nickel sensitivity was reportedly low in some studies of dyshidrosis patients but significantly elevated in other studies. Increased nickel excretion in the urine has been reported during exacerbations of pompholyx. Ingested metals have been found to provoke exacerbations of pompholyx in some patients.
- Low-nickel diets: These have reportedly decreased the frequency and severity of pompholyx flares. A high palmoplantar perspiration rate has been suggested to result in a local concentration of metal salts that may provoke the vesicular reaction. Contact allergy has been documented in 30% of patients with dyshidrotic eczema.
- Cobalt sensitivity: The oral ingestion of cobalt manifests systemic allergic dermatitis as dyshidrotic eczema less frequently than the oral ingestion of nickel. Much more common is the simultaneous occurrence nickel and cobalt allergy seen in 25% of nickel-sensitive patients developing pompholyx. In these cases, the eczema is usually more severe. When suspected as the cause of the dyshidrotic eczema, high oral ingestion of cobalt should be taken in consideration, regardless of the patch test results.3
- Low-cobalt diet: A point-based diet has been proposed to help patients limit cobalt ingestion and to keep the serum level below the threshold for developing flares, which is approximately less than 12 mcg/d. This diet has demonstrated higher compliance than an avoidance diet list. In addition, this diet also reduces the amount of nickel consumed.3
- Exposure to sensitizing chemicals or metals: Dyshidrotic eczema outbreaks are sometimes associated with exposure to sensitizing chemicals or metals (eg, chromium, cobalt, carba mix, fragrance mix, diaminodiphenylmethane, dichromates, benzoisothiazolones, paraphenylenediamine, perfumes, fragrances, balsam of Peru, Primula plant).
- Id reaction: Controversy surrounds the possible existence of an id reaction, which is considered to be a distant dermatophyte infection (tinea pedis, kerion of scalp) triggering a palmar pompholyx reaction (also termed pompholyx dermatophytid).
- Fungal infection: Pompholyx occasionally resolves when a tinea pedis infection is treated, then relapses when the fungal infection recurs, supporting the existence of this reaction pattern. Of patients who have a vesicular reaction to intradermal trichophytin testing, less than one third have experienced a resolution of pompholyx after treatment with antifungal agents.
- Emotional stress: This is a possible factor in dyshidrotic eczema. Many patients report recurrences of pompholyx during stressful periods. Improvement of dyshidrotic eczema using biofeedback techniques for stress reduction supports this hypothesis.
- UV-A light: A group of 5 patients with pompholyx developed typical lesions morphologically and histologically consistent with a vesicular dermatitis after a provocation with long-wavelength UV-A light. Of interest, UV-B phototherapy and photochemotherapy are well-known efficient therapies for pompholyx. Further studies ruled out contact dermatitis, polymorphic light eruption, and heat as the culprit of the lesions in these patients, confirming that the reaction was a true photosensitivity rather than a photoaggravation.14 Pompholyx caused by exposure to UV-A may be considered a variation of seasonal (summer) pompholyx.
- Other factors: Isolated reports describe other possible causative factors, such as aspirin ingestion, oral contraceptives, cigarette smoking, and implanted metals, among others. A 3-year prospective study of the causes of dyshidrotic eczema (pompholyx) in 120 patients found causes of pompholyx related to contact exposure (67.5%), including cosmetic products (31.7%) and metals (16.7%); interdigital-plantar intertrigo (10%); and internal causes (6.7%), with an additional 15% with undiagnosed (idiopathic) causes, probably related to atopic factors.15 Specifically, note the following:
- Contact allergy was found in 89 (74.2%) of 120 of the patients. The most frequent allergens were nickel, shower gel, chromium, fragrance, shampoo, and balsam of Peru. Less frequent allergens were lanolin, cobalt, thiuram, lauryl sulfate, fresh tobacco, p -phenylenediamine (PPD), formaldehyde, parabens, and octyl gallate. In 97 of 193 positive patch test results, correlation existed between the application of the agent and pompholyx recurrence. The relevance of the analysis was confirmed in 81 (67.5%) of 120 patients. In summary, the most frequent causes of pompholyx related to contact with substances were hygiene product intolerance (46.7%), metal allergy (25%), and others (28.3%).
- Intertrigo occurred in 19 (15.8%) of 120 patients. Of those, 80% presented with dermatophytosis and 20% presented with candidiasis. After 3 weeks of antifungal therapy, 6 of 19 patients remained symptomatic for pompholyx.
- With regard to internal causes, 30 patients presented with a positive patch test result for metals, but only 2 presented with exacerbations of the lesions after a challenge test.
- Of 58 patients with a history of smoking tobacco, 5 presented with a positive reaction, and 2 of those reactions were considered relevant.
- Drug allergy was determined to be the causative agent in 3 patients (amoxicillin in 2 and intravenous immunoglobulin in 1).
- Food-related pompholyx was detected in 4 patients, and after a challenge test, reactivation occurred in 3 patients (2 for paprika and 1 for orange juice).
Histologic Findings
Spongiosis with an epidermal lymphocytic infiltrate and intraepidermal vesicles or bullae are present. The vesicles are not associated with sweat glands.
Medical Care
Some mildly affected patients experience spontaneous resolution within 2-3 weeks. Biofeedback therapy for stress reduction has succeeded in some patients. Outpatient care is multifaceted.
The following treatment is appropriate if bullae are present:
- Use compresses with Burow solution (10% aluminum acetate) in a 1:40 dilution until bullae resolve (usually, within a few days).
- Compresses with a 1:10.000 solution of potassium permanganate are also effective.
- Drain large bullae with a sterile syringe, and leave the roof intact.
- Prescribe systemic antibiotics that cover Staphylococcus aureus and group A streptococci.
Topical corticosteroids are the mainstay of treatment. Typically, use class I steroids initially, then class II or III steroids. Ointments penetrate skin better than creams; patients may prefer creams during the day. Topical antipruritics with pramoxine are useful.
Systemic corticosteroids can also be used. Either oral prednisone or intramuscular triamcinolone suspension may be used for severe episodes. Tapering of prednisone can follow intramuscular treatment.
Topical calcineurin inhibitors may be helpful. Some patients may benefit from topical tacrolimus or pimecrolimus. Several studies have demonstrated their efficacy and tolerability in the treatment of chronic hand dermatitis,17 and long-term occlusive therapy has also been determined to be efficacious, particularly in persons with severe dyshidrotic eczema.17 Advantages of topical calcineurin inhibitors over topical corticosteroids include the lack of development of tachyphylaxis, telangiectasias, and thinning and atrophy of the skin.18 Personal experience of the coauthor shows effective control in several patients followed in her practice with topical calcineurin inhibitor therapy alone. Note that topical calcineurin inhibitors can exacerbate irritant hand dermatitis.
UV-A or UV-A1 alone or with oral or topical psoralen has been used. Hand and/or foot UV-A therapy (UV-A or UV-A1 alone or with oral or topical psoralen) improves the eruption and pruritus when administered 2-3 times per week. The dose typically starts at 0.5 J per treatment and is increased by 0.5 J at every other or every third treatment.19,20
8-Methoxypsoralen (MOP) plus UV-A (bath-PUVA) is an option. Topical application of MOP and UV-A (bath-PUVA) has been demonstrated to be the preferred method for the treatment of dyshidrotic eczema compared with oral PUVA.21 Local narrow-band UV-B has been shown to be as effective as bath-PUVA in patients with chronic hand eczema of dry and dyshidrotic types.22
Botulinum toxin A injections may be helpful in some patients. Botulinum toxin A intradermal injections as an adjuvant to topical corticosteroids has been tested in a study in which 6 patients who completed an 8-week trial achieved significant reductions in the Dyshidrotic Eczema Area and Severity Index (DASI) scores and faster reductions of pruritus and vesiculation.18 In another study, 7 of 10 vesicular pompholyx patients achieved good-to-very good responses after the injection of botulinum toxin A alone, with a reduction of pruritus.23
For severe refractory pompholyx, azathioprine, methotrexate24 mycophenolate mofetil, cyclosporine,25 or etanercept may be helpful. Etanercept has been administered subcutaneously to one patient with recalcitrant hand pompholyx at a dose of 25 mg twice a week. The patient achieved complete remission for 4 months, after which the patient had a relapse. The etanercept dose was increased to 50 mg twice a week without improvement.26 Consider measuring thiopurine methyltransferase levels, which may help guide azathioprine therapy. Accurate dosing avoids both toxicity and underdosing.
Nickel chelators, such as disulfiram (Antabuse), occasionally are used in nickel-sensitive patients who demonstrate a positive oral provocation test.27
Tap water iontophoresis with pulsed direct current may be helpful as adjuvant treatment.28
Khellin, a furanochromone similar to methoxypsoralen, may be used in combination with photochemotherapy (sun exposure) for recalcitrant palmoplantar cases.29 Khellin, unlike other psoralens, does not induce skin phototoxicity (erythema) and hyperpigmentation of healthy skin after UV-A radiation therapy.
Alitretinoin (9-cis retinoic acid) activates the retinoid X receptor and all retinoic receptors. Note the following from clinical trials:
- It has been studied in 319 patients with chronic hand dermatitis (70 with pompholyx) refractory to standard therapy in a randomized, double-blind, placebo-controlled, multicenter trial in which oral alitretinoin was administered at doses of 10 mg, 20 mg, or 40 mg once daily of for 12 weeks. Although alitretinoin induced a significant clinical improvement in a dose-dependent fashion (53% improvement in disease status and 70% reduction in clinical features), no difference was noted in the group of patients with pompholyx compared with placebo.18,30
- In another randomized, double-blind, placebo-controlled, multicenter trial, oral alitretinoin showed a response rate of 33% at a dose of 30 mg/d, compared with 23% at a dose of 10 mg/d and 16% with placebo in 377 patients with pompholyx.31
- Headache and mucocutaneous adverse events, including dry skin, rash, alopecia, exfoliative dermatitis, and hyperlipidemia, were the most common adverse events in these trials.
- Alitretinoin 1% gel has been evaluated for the treatment of classic Kaposi sarcoma,32 photoaging,33 pyogenic granuloma,34 and cutaneous T-cell lymphoma.35 Currently, alitretinoin 1% gel has not been used for the topical treatment of pompholyx.
- Some data suggest that alitretinoin may be effective and well tolerated for severe chronic hand eczema. Three phase III studies, 2 double-blind randomized controlled trials, and an open-label study evaluated safety36 and efficacy37 of once-daily oral alitretinoin at 10 mg or 30 mg versus placebo in 1032 patients with chronic hand eczema, including pompholyx, in whom treatment with potent topical corticosteroids had failed. According to physician assessment, “clear” or “almost-clear” status was achieved in up to 48% of patients in the alitretinoin groups and 17% in the placebo group (P <.001). Median percentage reduction in disease symptoms was 75%. Alitretinoin at 30 mg had responses faster (median 85 d) than placebo (median 141 d) (P <.001). Among complete responders who relapsed, 80% in the alitretinoin groups responded to the same alitretinoin dose and 8-10% of patients in the placebo group responded to retreatment with placebo.
- Common adverse effects included headache, flushing, erythema, and xerosis. Headache was the most common adverse effect with alitretinoin at 30 mg. Also in the treatment group, dry skin, dry eyes, dry mouth, dry lips, and cheilitis were reported in 10% of patients, compared with 4% of patients in the placebo group. Lipid abnormalities were similar to those seen with other retinoids.
- Currently, another phase III, randomized, double-blind (subject, investigator), placebo-controlled, parallel-assignment, safety/efficacy study is being conducted on the treatment of chronic hand dermatitis (including pompholyx) using oral alitretinoin at 30 mg/d (1 capsule) for up to 24 weeks; the estimated completion date is 2010.38 Also see Efficacy and Safety of a Retinoid in the Treatment of Severe Chronic Hand Eczema (HANDEL).
Newer and potential agents for pompholyx, such as topical bexarotene, systemic alitretinoin, leukotriene receptor antagonists, leukotriene synthesis inhibitors, phosphodiesterase-4 inhibitors, and monoclonal antibodies, have shown to be effective for the treatment of chronic hand dermatitis and other inflammatory conditions, including atopic dermatitis. Controlled studies need to be conducted to establish their efficacy and safety for the treatment of dyshidrotic eczema (pompholyx).