|
Graft versus host disease =داء رفض الطعم للمضيف |
 |
 |
 |
|
Graft Versus Host Disease
|
|
GVHD occurs in situations in which donor immunocompetent T cells transferred into allogenic hosts are incapable of rejecting them. The sources of the T cells include primarily peripheral blood stem cell and bone marrow transplants and,
|
|
infrequently, unirradiated blood products , solid organ transplants , and matemal-fetallymphocyte engraftment. Graft-versus-host-like reaction has been reported in patients with a thymoma or lymphoma .
|
|
The disease can be divided into an acute and a chronic phase. Acute GVHD typically occurs between 7 and 21 days after transplantation but may be seen as late as 3 months; chronic GVHD arises after a mean of 4 months but may occur as soon as 40 days posttransplantation. The two phases were originally defined on the basis of time of presentation . However, the use of donor lymphocytes and the withdrawal of immunosuppression in relapsed patients have obscured these time-based divisions. In addition, many patients have both phases, either merging with one another or separated by an asymptomatic period. The frequency of acute GVHD depends on the disparity of HLA antigens . The risk of chronic GVHD is 11 times greater if the patients had prior acute GVHD.
|
|
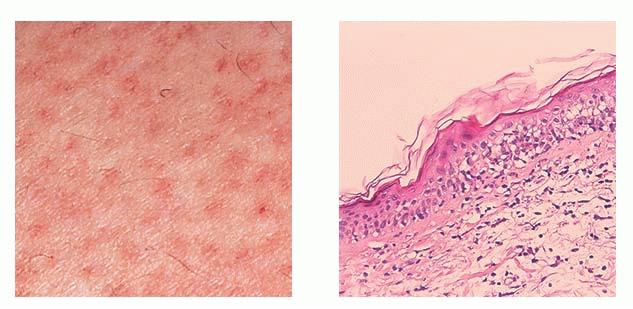
In the acute phase, the classic triad includes skin lesions, hepatic dysfunction, and diarrhea. The clinical severity is judged on the extent of the cutaneous eruption, total bilirubin, and stool volume. The eruption is characterized by extensive macular erythema, a morbilliform eruption, purpuric lesions, violaceous scaly papules and plaques, bullae, or in rare cases a TEN-like epidermal detachment. There is a predilection for the cheeks, ears, neck, upper chest, and palms and soles. Occasionally, follicular papules are seen simulating a folliculitis. Oral lesions may be present. About 30% of patients die from complications of acute GVHD. The overall clinical stage, during the first 40 days after transplantation, is useful in identifying patients with progressive and fatal disease . Cutaneous GVHD may be due to a synergistic effect from local irradiation .
In the chronic phase, an early lichenoid stage and a late sclerodermoid stage can be distinguished. Each stage can occur without the other. Although usually generalized, the involvement is in rare instances localized to a few areas. In the lichenoid stage, both the cutaneous and oral lesions may be clinically similar to those in lichen planus. In addition, the skin may show extensive erythema and irregular hyperpigmentation. A poikiloderma phase may precede the eventual sclerodermoid stage . Other late manifestations include a lupus erythematosus-like eruption, cicatricial alopecia, chronic ulcerations, pyogenic granuloma, and angiomatous lesions .
|
|
histopathology
the early changes in the acute phase consist of focal basal vacuolation and sparse superficial
|
|
perivascular lymphocytic infiltrate with exocytosis of individual cells into the epidermis and follicular epithelium. The number of lymphocytes correlates positively with the probability of developing more severe acute GVHD . In association with the perivascular infiltrate, there is marked endothelial cell swelling and narrowing of the vascular lumen. Established lesions show more pronounced vacuolation, focal spongiosis, lymphocytic infiltration, and dyskeratosis at all levels of epidermis. The acute phase has been divided into four histopathologic grades . In grade 1 disease, there is focal or diffuse vacuolization of the basal cell layer. In grade 2 lesions, spongiosis and dyskeratotic keratinocytes are identified , with some accompanied by two or more epidermal lymphocytes, a phenomenon known as satellite cell necrosis. The necrotic keratinocytes contain a pyknotic nucleus and eosinophilic cytoplasm. Grade 3 lesions are characterized by subepidermal cleft formation. In grade 4, there is complete loss of the epidermis. In cases with follicular papules, the involved follicles show degenerate changes in the cells of the follicular epithelium similar to those in the epidermis. In rare cases, basal vacuolization and dyskeratosis of the follicular epithelium may be the only changes .
In the chronic phase, the early lichenoid stage may still show evidence of satellite cell necrosis within the epidermis . The overall histologic picture greatly resembles that of lichen planus with hyperkeratosis, hypergranulosis, acanthosis, apoptotic keratinocytes, and a mononuclear cell infiltrate immediately below the epidermis with pigmentary incontinence. As in lichen planus, apoptotic keratinocytes may "drop" into the upper dermis. There may be areas of separation of the basal cell layer from the dermal papillae resembling the clefts seen in severe lichen planus. A rare manifestation is so-called columnar epidermal necrosis, characterized by small foci of total epidermal necrosis accompanied by a lichenoid tissue reaction .
|
|
In the late sclerodermoid phase, the epidermis is atrophic, with the keratinocytes being small, flattened, and hyperpigmented. Basal layer vacuolization, inflammation, and colloid body formation are rare or absent. The dermis is thickened, with sclerosis extending into the subcutaneous tissue resulting in septal hyalinization. The adnexal structures are destroyed . Subepidermal bullae were present in one reported case.
|
|
IF Testing. Epithelial basement membrane zone granular IgM and complement deposition is present in 39% of patients with the acute form and in 86% of patients with the chronic form of GVHD. In addition, IgM and C3 have been found in the walls of dermal vessels.
|
|
Pathogenesis.
Acute and chronic forms of the disease have a different pathogenesis. In acute GVHD, it is believed that preparative regimen before the infusion of the graft causes extensive tissue damage, which releases inflammatory cytokines and exposes recipient major histocompatibility complex (MHC) antigens. Recognition of the host antigen by donor T cells and activation and proliferation of them is crucial in the initial phase.
|
|
The greater the disparity between donor and recipient MHC, the greater the T-cell response. In identical pairs, the donor T cells recognize minor antigen difference. Infiltration of both CD4+ and CD8+ T cells or with either one of them predominating has been reported yfJ T cells represent a minority of infiltrates . B cells are not found.
|
|
The inflammatory cytokines (ILs, GM-CSF, TNF-a IFN-y) produced by activated T cells and by tissue damage during the preparative regimen also activate mononuclear phagocytes and NK cells (180). Both Fas/FasL-dependent apoptosis and perforin/granzyme-dependent killing are important in GVHD-induced damage . In skin, young rete ridge keratinocytes, follicular stem cells , and Langerhans cells are preferred targets. However, the exact
|
|
mechanisms by which the skin, liver, and gastrointestinal tract are targeted are not clear.
|
|
Less is understood about the pathophysiology of chronic GVHD. The role of donor T cells against the recipient's tissue has been demonstrated. In addition, autoreactivity has also been suggested. Most immunohistochemical studies have shown that CD8+ T cells predominate. Tumor necrosis factor-a and IL-1a are constantly produced by keratinocytes in the lesional skin .
Ultrastructural Study.
The necrotic keratinocytic cytoplasm is filled with numerous aggregated tonofilaments. Granule-producing cytotoxic lymphocytes, NK-like cells, have been identified in direct cytolytic attack on epithelial cells undergoing apoptosis.
|
|
Differential Diagnosis.
The acute phase of GVHD is similar to EM, with scattered necrotic keratinocytes and the formation of subepidermal clefts through hydropic degeneration of basal cells. In severe cases, the fulminant lesions resemble TEN. These patients are also at increased risk for drug eruptions, chemotherapy-induced eruptions, and radiation dermatitis, all of which may be indistinguishable from acute GVHD. If there is follicular dyskeratosis, the diagnosis is much more likely to be acute GVHD. The presence of eosinophils is not necessarily in favor of drug reaction, as eosinophils are occasionally observed in GVHD. Epidermal changes identical to acute GVHD may be seen in bone marrow transplant patients without cutaneous lesions.
|
|
The eruption of lymphocyte recovery occurs predominantly in patients after receiving cytoreductive therapy (without bone marrow transplant) for acute myelogenous leukemia. The eruption is typically morbilliform and develops between 6 and 21 days of chemotherapy, correlating with the earliest recovery of lymphocytes to the circulation. In contrast to patients with GVHD, these patients do not develop diarrhea or liver abnormalities. Resolution occurs over several days. Histopathologically, a superficial perivascular mononuclear cell infiltrate, basal vacuolization, spongiosis, and rare dyskeratotic keratinocytes are present. The changes may be indistinguishable from those of early allogeneic or autologous GVHD, and clinical information is essential (184). The systemic administration of recombinant cytokines prior to marrow recovery leads to a relatively heavy lymphocytic infiltrate with nuclear pleomorphism and hyperchromasia .
|
Distinguishing between the lichenoid lesions of GVHD and lichen planus is often impossible. However, late sclerotic lesions can be differentiated from scleroderma by the marked atrophy of the epidermis. Active synthesis of collagen takes place largely in the upper third of the dermis; in scleroderma, collagen is synthesized mainly in the lower dermis and in the subcutaneous tissu
|
|
|
|