


ERYTHEMA INFECTIOSUM AND
PARVOVIRUS B19 INFECTION
Epidemiology
Erythema infectiosum (fifth disease) is worldwide in distribution, can occur throughout the year, and can affect all ages. It tends to occur in epidemics, especially associated with school outbreaks in the late winter and early spring. Serologic studies show increasing prevalence of antibodies with age. Various studies indicate that from 15 percent to 60 percent of children 5 to 19 years of age and 30 percent to 60 percent of adults are seropositive. Seroprevalence increases to greater than 90 percent in the elderly. Previous infection with B19 seems to confer lifelong immunity.
PARVOVIRUS B19 AT A GLANCE
· Causes erythema infectiosum, fifth disease.
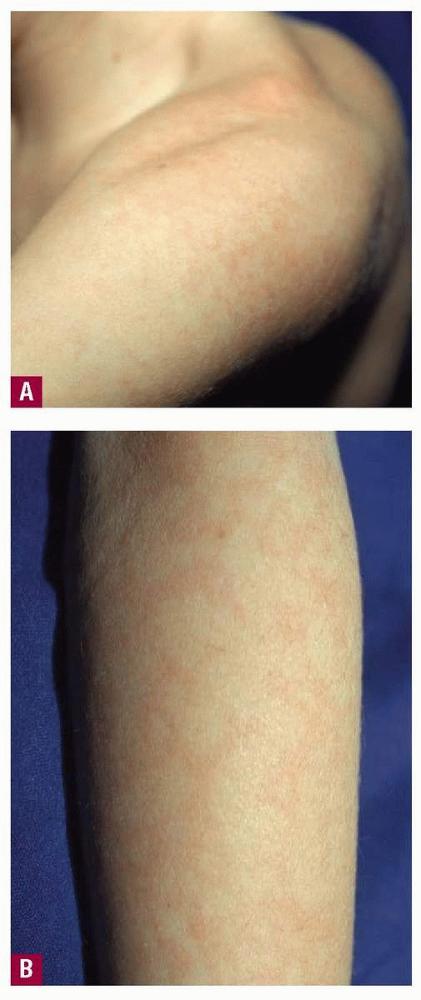
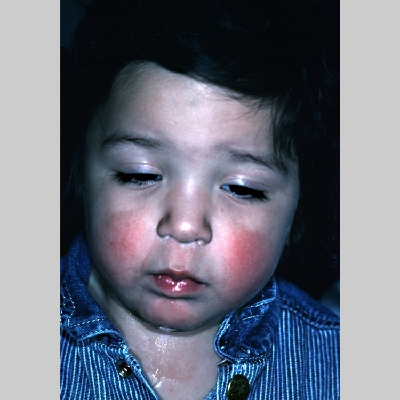
· Fifth disease in children with “slapped cheeks” followed by an erythematous, lacy eruption on the trunk and extremities.
· Symmetric polyarthritis, particularly of the small joints.
· Causes papular purpuric gloves-andsocks syndrome with pruritic erythema, edema, and petechiae of the hands and feet, fever, and oral erosions in adolescents.
· Aplastic crisis in patients with increased red blood cell turnover, chronic anemia in immunocompromised persons, and fetal hydrops.
The incubation period for erythema infectiosum is from 4 to 14 days. After intranasal inoculation of parvovirusinfected serum to healthy volunteers, low-grade fever and non-specific complaints occurred at the time of viremia, 6 to 14 days after inoculation, and the rash appeared at day 17 or 18.
Parvovirus B19 is thought to be transmitted primarily by the respiratory route via droplet aerosol during the viremic phase, and B19 DNA has been found in respiratory secretions of viremic patients. After the rash of erythema infectiosum appears, B19 is not found in respiratory secretions and is usually not present in the serum. This suggests that persons with erythema infectiosum are infectious only before the onset of the rash.
The virus seems to be effectively spread after close contact. The secondary attack rate among susceptible household contacts is approximately 50 percent. Transmission may occur via blood transfusion, from blood products, and vertically from mother to fetus. The transmission of B19 through blood transfusion is particularly problematic because the nonenveloped virus is not killed by the solvent detergents or heat that are used to inactivate HIV and hepatitis viruses.
Etiology and Pathogenesis
The B19 virus belongs to the family Parvoviridae and the genus Parvovirus. B19 lacks an envelope and contains single-stranded DNA. It is the smallest single-stranded DNA-containing virus known to infect humans, measuring 18 to 26 µm in diameter. Parvoviruses are widespread in veterinary medicine, but animal parvoviruses are not thought to be transmissible to humans.
The pathogenesis of erythema infectiosum is unknown, but the mechanism may involve immune complexes. The more serious manifestations of parvovirus infection relate to the fact that the virus infects and lyses erythroid progenitor cells. Evidence suggests that the blood group P antigen (globoside) is a receptor of parvovirus. Because some individuals lack P antigen, they are not susceptible to infection with B19. In patients with increased red blood cell destruction or loss who depend on compensatory increase in red cell production to maintain stable red cell indices, B19 infection may lead to transient aplastic crisis. Such patients include those with anemia associated with acute or chronic blood loss. When parvovirus infects the erythroblasts in a developing fetus with decreased red cell survival, the result may be hemolysis and anemia. Anemia may trigger congestive heart failure, edema (fetal hydrops), and possibly fetal death.
Clinical Findings
PARVOVIRUS B19 IN CHILDREN
Most infections caused by B19 are asymptomatic and unrecognized. Fifth disease, the most common clinical picture associated with the virus, usually begins with non-specific symptoms such as headache, coryza, and low-grade fever approximately 2 days before the onset of the rash. Patients may have headache, pharyngitis, fever, malaise, myalgias,
coryza, diarrhea, nausea, cough, and conjunctivitis coinciding with the rash. Approximately 10 percent of children with erythema infectiosum develop arthralgias or arthritis. Large joints are affected more often than small joints. Occasionally, children may present with chronic joint complaints suggestive of juvenile rheumatoid arthritis.
The characteristic rash begins with confluent, erythematous, edematous plaques on the malar eminences, the “slapped cheeks” As the facial rash fades over 1 to 4 days, pink to erythematous macules or papules appear on the trunk, neck, and extensor surfaces of the extremities. These lesions have some central fading, giving them a lacy or reticulated appearance The rash can be morbilliform, confluent, circinate, or annular, and there have been reports of palmar and plantar involvement. The eruption typically lasts 5 to 9 days, but can recur for weeks or months with triggers such as sunlight, exercise, temperature change, bathing, and emotional stress. In some outbreaks, pruritus is a major feature of the rash in children.
There have been occasional reports of parvovirus B19 associated with vascular purpura, including Henoch-Schönlein purpura. An enanthem consisting of erythema of
the tongue and pharynx and red macules on the buccal mucosa and palate can occur.
PARVOVIRUS B19 IN ADULTS
Acute arthropathy is the primary manifestation of B19 viral infection in adults. It occurs mainly in women and affects the small joints of the hands, the knees, other joints, such as the spine and costochondral joints, are involved. This symmetric polyarthritis is usually of sudden onset and is self-limited but can be persistent or recurrent for months. It may mimic Lyme arthritis or rheumatoid arthritis.
The constitutional symptoms are usually more severe in adults than in children. Fever, adenopathy, and a mild arthritis without a rash is the usual course. Women are more likely than men to have joint complaints and rash, whereas men often present with only a flu-like illness. Some adults may have fatigue, malaise, and depression for weeks after the infection. Asymptomatic infection can certainly occur in adults as well as in children. In one outbreak, 26 percent of adults were reported to be asymptomatic. Parvovirus B19 can cause numbness and tingling of the fingers with or without other features of fifth disease. Pruritus that is sometimes severe can occur with or without a rash. It has been suggested that if pruritus is a complaint in a patient with acute-onset arthritis, parvovirus should be considered as a possible cause.
The rash in adults, if present at all, is usually macular and blotchy or lacy, often on the extremities, and rarely demonstrates the characteristic slappedcheek appearance. Other cutaneous manifestations associated with B19 infection in adults include purpura, vesicles and pustules, palmo-plantar desquamation, a morbilliform exanthem with Koplik spots, and livedo reticularis.