|
Subacute Cutaneous Lupus Erythematosus SCLE = الذئبة الحمامية الجلدية تحت الحادة |
 |
 |
 |
                                                                      
Lupus Erythematosus, Subacute
Cutaneous
Subacute cutaneous lupus erythematosus (SCLE) is a nonscarring non–atrophy-producing photosensitive dermatosis. SCLE may occur in patients with systemic lupus erythematosus (SLE), Sjögren syndrome, and deficiency of the second component of complement (C2d), or it may be drug induced. Some patients also have the lesions of discoid lupus erythematosus (DLE), and some may develop small vessel vasculitis.
Patients with SCLE frequently fulfill 4 or more of the criteria used to classify SLE (see Systemic Lupus Erythematosus). Serologic abnormalities are common. Therapy with sunscreens, topical corticosteroids, and antimalarial agents is usually effective.
SCLE occurs in genetically predisposed individuals, most often in patients with human leukocyte antigen B8 (HLA-B8), human leukocyte antigen DR3 (HLA-DR3), human leukocyte antigen DRw52 (HLA-DRw52), and human leukocyte antigen DQ1 (HLA-DQ1). A strong association exists with anti-Ro (SS-A) autoantibodies. The reaction is believed to be related to ultraviolet (UV) light modulation of autoantigens, epidermal cytokines, and adhesion molecules, with resultant keratinocyte apoptosis.
Worldwide, SLE prevalence ranges from 17-48 cases per 100,000 persons. The highest prevalence of SLE occurs in patients aged 40-60 years. The male-to-female ratio of SLE is approximately 1:10. The male-to-female ratio of cutaneous lupus erythematosus (CLE) is approximately 1:2-3. Of patients with CLE, 10-50% have SCLE.
No differences in the prevalence of this disorder are recognized between the United States and other countries.
Approximately one half of patients with SCLE have 4 or more of the criteria for classification as SLE, but in these patients, the disease is less severe, although in individual patients the full range of severity and end organ dysfunction is possible. By definition, skin lesions heal without scarring or atrophy but may leave residual dyspigmentation.
SCLE is more common in whites (85%).
Male-to-female ratio of SCLE is 1:4.
SCLE typically occurs in patients aged 15-70 years. The mean age is approximately 43 years.
- Subacute cutaneous lupus erythematosus (SCLE) often begins as a papular eruption.
- Papules may show a photosensitive distribution. Many patients notice that sun exposure results in an exacerbation of their disease, and some report worsening each spring and summer.
- Patients may complain of mild pruritus, but most patients are asymptomatic.
- Eventually, lesions develop into annular erythema or become psoriasiform in character.
- SCLE may wax and wane.
- Approximately 50% of SCLE patients have accompanying joint involvement.
- Arthralgias are common, often symmetrical, and usually affect small joints such as hands and wrists.
- Arthritis may occur but is unusual (<2%).
- Patients commonly complain of fatigue.
- Some patients have Sjögren syndrome, while others note dryness of their eyes and mouth.
- Patients may manifest symptoms of SLE; therefore, the history should include an assessment for symptoms of pleuritis, pericarditis, neurologic involvement, and renal impairment.
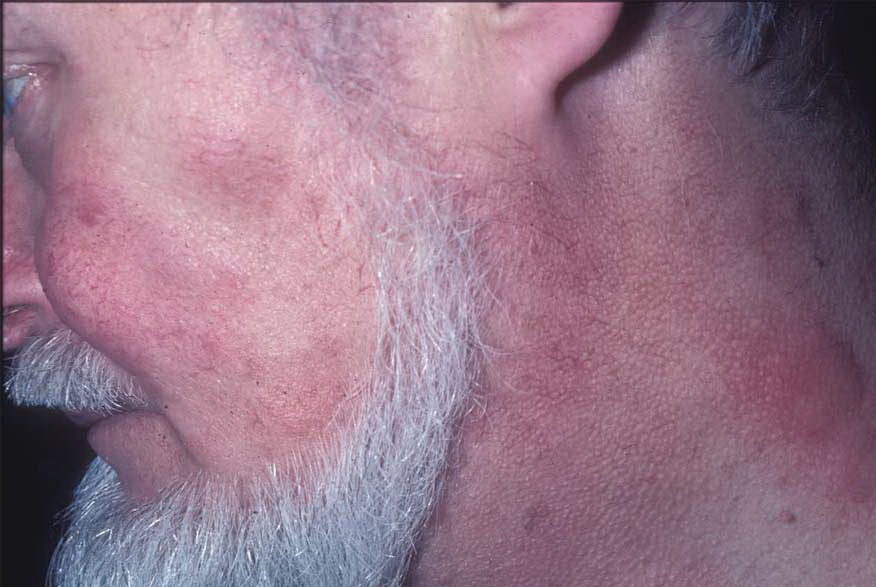
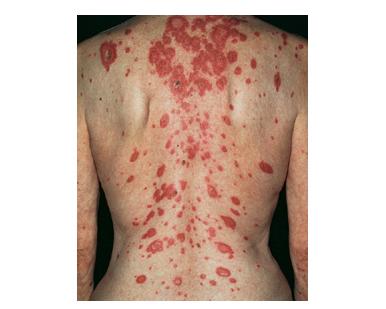
- The primary lesion of subacute cutaneous lupus erythematosus (SCLE) is an erythematous papule or a small plaque with a slight scaling . Primary lesions expand and may merge and eventually form either plaques with scaling in the papulosquamous variant or annular and/or polycyclic lesions in the annular variant .
- Papulosquamous lesions may mimic psoriasis or lichen planus, while annular lesions may mimic erythema annulare centrifugum. Most patients exhibit one predominant type of lesion, and some also manifest isolated lesions of DLE.
- SCLE lesions primarily are photodistributed. When they occur on the lower extremities, they often are purpuric.
- Early lesions of SCLE may be difficult to distinguish from polymorphous light eruption (PMLE). In this author's opinion, PMLE and SCLE are distinctive disorders, but patients with recurrent photosensitive pruritic eruptions who are anti-Ro (SS-A) positive blur the distinction and might well be better classified as having SCLE rather than believed to have both disorders, as has been suggested by some investigators in Europe.
- Several unusual variants of SCLE have been reported.
- Tumid lupus erythematosus (TLE) involves a deeper more nodular lesion in which little or no scaling is seen . Some authorities have suggested that this variant is better classified as chronic cutaneous lupus erythematosus, while others have pointed out that this variant does not demonstrate an interface dermatitis upon histopathological evaluation and therefore belongs in a separate subset among the skin lesions that are not histopathologically specific.
-
- Annular erythema of Sjögren syndrome has been reported in Japanese and Polynesian patients. The author believes this is not a distinct entity, but rather SCLE with Sjögren syndrome in a particular ethnic population.
- A variant including erythema multiforme–like lesions in association with DLE and chilblains may exist, but it is not clear whether this is a distinct entity.
- Patients with SCLE may have arthritis and pleuritis or pericarditis that manifest physical findings on joint or cardiopulmonary examination, respectively. Patients also may have nonspecific cutaneous manifestations of lupus erythematosus (LE), such as livedo reticularis, palpable purpura, urticaria, ischemic changes of the distal fingertips (resulting from Raynaud phenomenon), or mucosal leukoplakic or ulcerative lesions.
- Neonatal lupus erythematosus (NLE) most often manifests as a nonscarring form of LE . Skin lesions are worsened by UV light and usually resolve by age 4-6 months. Some patients with NLE have congenital heart block. Patients with complete heart block eventually may require a pacemaker, may die suddenly, or may develop heart failure. NLE also may be manifested by cytopenias, and if thrombocytopenia is present, the neonate may have petechiae. Lastly, hepatosplenomegaly also may occur. Except for congenital heart block, all other manifestations resolve without intervention within 4-6 months.
- Patients are predisposed genetically to develop subacute cutaneous lupus erythematosus (SCLE).
- Usually, the disease manifests following UV light exposure, but other triggers or inciting factors also must be implicated.
- Exacerbation of disease or induction of lesions most commonly follows UV-B exposure. Some patients exhibit sensitivity to only UV-A or to both UV-A and UV-B.
- Several drugs may induce SCLE; the most frequently implicated is hydrochlorothiazide. Many pharmaceutical companies combine an antihypertensive agent with hydrochlorothiazide, and this should be assessed carefully. Additionally, implicated agents include calcium channel blockers, angiotensin-converting enzyme inhibitors, terbinafine, and tumor necrosis factor antagonists. Therefore, a careful drug history should be part of the initial evaluation of patients with SCLE.7
- Patients with a deficiency of the second component of complement (C2d) often manifest SCLE lesions as part of the SLE-like disease.
|
|
|
|