|
Trichotillomania
Trichotillomania is a condition in which patients pull or manipulate hair from the scalp or other body sites . For example, persistent rubbing of an area of the scalp that may be pruritic or compulsive avulsion of hair shafts can lead to zones of alopecia characterized by sparse, ragged, broken stubble. Hair shaft breakage and loss may
|
|
be associated with damage to the scalp, as evidenced by erosions or crusts. Trichotillomania occurs most often in children and adolescent girls. In children under the age of 6 years, the disorder may be more benign and selflimited . In teens and adults, trichotillomania is more likely to be associated with psychopathology. It has features in common with obsessive-compulsive disorder , and in one study a large proportion of patients with trichotillomania also had comorbid self-injurious habits . Trichotillomania is part of the Diagnostic and Statistical Manual of Mental Disorders, fourth edition, classification of psychiatric disorders . Treatment of this form is often difficult; conventional modalities that may be tried include antidepressant or psychotropic medications, topical adjunctive therapies, and psychotherapy . Concomitant alopecia areata has been reported .
|
|
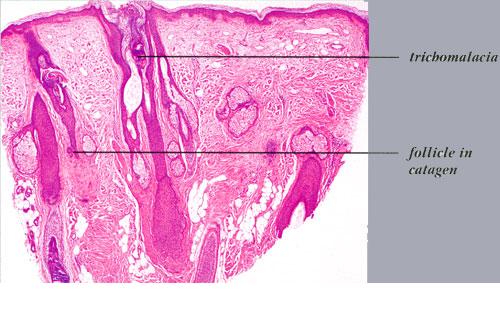
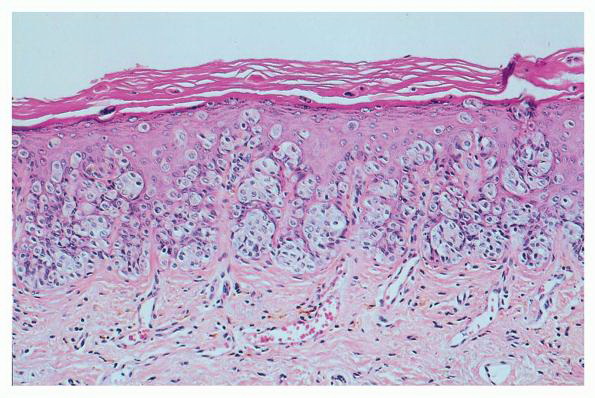
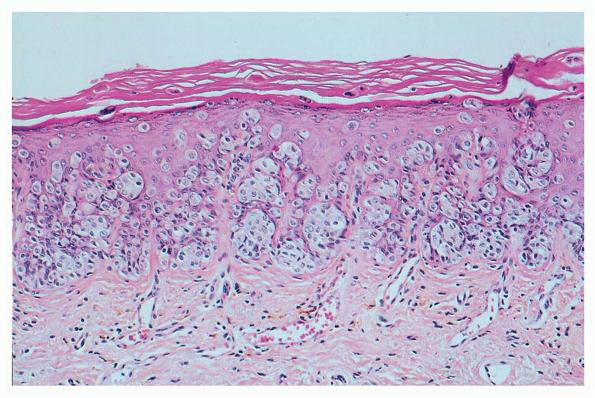
Because not all follicles in a given area are affected, transversely sectioned scalp biopsies may increase the yield of finding the diagnostic histologic features of trichotillomania, including increased numbers of catagen and telogen hairs (most cases) and empty or distorted follicles (greater than 50% of cases) (194). The same study found pigment casts and trichomalacia in less than 50% of cases. When the scalp is also rubbed persistently, epidermal changes of lichen simplex chronicus may be seen in vertical sections.
|
|
The histologic differential diagnosis of increased numbers of catagen and telogen hairs, characteristic of trichotillomania, includes alopecia areata and telogen effluvium. Trichotillomania also shares with early alopecia areata the features of normal hair density and occasional trichomalacia, but trichotillomania lacks the follicular miniaturization and peribulbar infiltrates. In telogen effluvium, evidence of trauma to follicles, as discussed earlier, is not seen. The histologic findings in early traction alopecia are said to be identical with those of trichotillomania, but fewer follicles are involved and the features are less prominent (see later discussion) .
|
|
Traction Alopecia
Traction alopecia is another type of mechanical alopecia, usually resulting from a variety of hair-styling practices, particularly in African-Americans, that includes tight braids, corn rows, straightening, and the use of sponge rollers . Hair follicle injury is similar to that produced in trichotillomania, but in traction alopecia there are differences that relate to the use of less force over a greater period of time (194). Traction alopecia is often classified clinically and histologically as "early" and "late" disease . In early disease, tension on hair follicles exists over the course of months to a few years, sometimes presenting as a traction folliculitis with perifollicular erythema and pustules . In late disease, hair is subject to traction over many years. In early disease, discontinuation of the abnormal forces on the hair leads to regrowth of hair, but in late disease, follicles are lost, producing a permanent alopecia. Early and late disease are commonly found together in the same patient; as permanently scarred areas develop (late disease), terminal hairs at the periphery are used in styling, becoming the new target of traction (early disease) (. Occupationally related traction alopecia has been reported due to wearing of a nurse's cap, occurring at the site of pin placement used to secure the cap .
Histopathology.
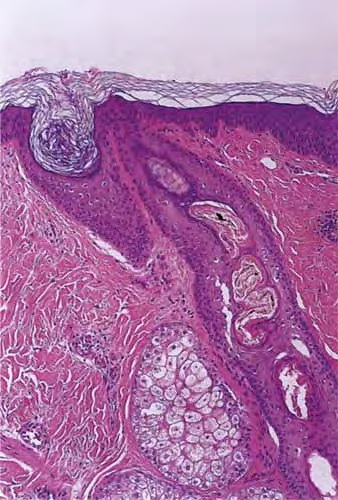
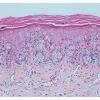
In early traction alopecia, the histologic findings are similar to those of trichotillomania, albeit more subtle (194). For instance, the density of follicles is normal, with a normal number of vellus hairs. Premature conversion of anagen hairs to catagen occurs, resulting in an increased number of catagen and telogen follicles. Pigment casts and trichomalacia are sometimes found, although less often than in trichotillomania. Inflammation is absent.
|
|
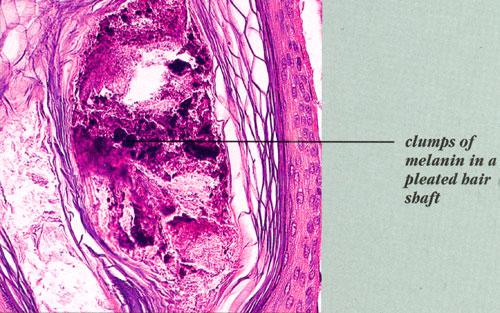
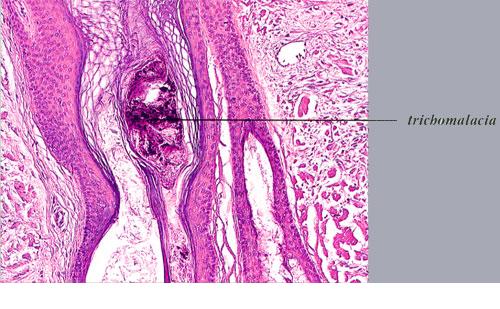
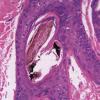
being deposited distally as the hair is plucked {194}. Pigment casts are due to injury to the hair matrix, although some authors have theorized that they result from the sudden conversion of anagen to catagen . Hair shaft changes, termed trichomalacia, may be seen. Characterized by diminished size, distorted and odd shape, and irregular pigmentation of the shaft, trichomalacia is additional evidence of trauma to the matrix . Traumatized follicles can also show considerable distortion of the bulbar epithelium and conspicuous hemorrhage .
|
|
Pigment casts, which are clumps of melanin pigment, may be seen in the hair papilla and peribulbar connective tissue. They are also commonly seen in the upper portion of the hair follicle as a result of pigmented matrical cells
|
|
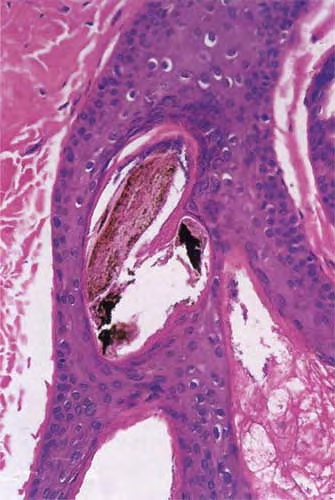
Histopathology. In horizontally sectioned biopsies of trichotillomania uncomplicated by the coexistence of other types of alopecia, the density of hair follicles is normal, as is the terminal-to-vellus hair ratio. The diagnostic finding, when seen, is distorted hair follicle anatomy, without inflammation . Specifically, the pulling of hairs can leave behind empty anagen follicles and "torn-away" follicles, the result of plucked hair shafts that retain parts of the hair matrix and root sheaths . Additional microscopic evidence of traumatic injury was published by Royer et al. as the "hamburger sign," describing a vertically oriented split in the hair shaft containing proteinaceous material and erythrocytes, resembling a hamburger within a bun . Damaged follicles enter the resting phase, leading to an increase in the percentage of catagen and telogen hairs, as high as 75% . Often the hairs do not become normal catagen hairs and appear distorted and abnormal .
|
|
outnumbering terminal follicles. In late
|
|
disease, the pathology shows an "end-stage" scarring alopecia, a histologic picture shared by many forms of permanent alopecia at an advanced stage. Pigment casts and trichomalacia are not seen in late traction alopecia.
|
|
Anagen Effluvium
Acute loss of actively growing (anagen) hairs occurs as a result of a severe insult that disrupts the mitotic activity of dividing cells in the hair matrix , with hair shaft production suffering greatly. The shaft becomes tapered proximally, breaks at the narrowest point, and is shed. The most commonly encountered forms of anagen effluvium are from chemotherapeutic agents and radiation therapy , although heavy metal poisoning and other toxins should be considered (262). Rapidly progressing alopecia totalis may present as anagen effluvium.
|
|
Microscopic Examination of Hairs. Diagnosis of anagen effluvium is usually made on clinical grounds with the aid of a trichogram or gentle hair pull, so that scalp biopsies are seldom done. Resting (telogen) hairs are immune to the metabolic insult, so that when sufficient anagen hairs are lost through shedding, a forcible hair pluck performed late in the course of disease will show almost all telogen hairs; a telogen count that approaches 100% on trichogram is a clue that a type of anagen effluvium is to blame. Early, a gentle hair pull demonstrates "pencilpoint" tapered hairs with a pointed or frayed end (.
|
|
In contrast, in loose anagen syndrome, the proximal portion of pulled anagen hairs shows a ruffled hair shaft cuticle because the inner and outer root sheaths are lost during extraction (. One report described the loss of normal-appearing anagen hairs with an intact inner root sheath and partially intact outer root sheath in the setting of pemphigus vulgaris, in which the cleavage plane is in the outer root sheath .
|
|
Telogen Effluvium
Effluvium is a Latin term meaning "a flowing out" . Telogen effluvium results from "outflowing," or shedding, of hair shafts in the telogen phase of the hair growth cycle. The concept was originally delineated by Kligman . This condition has many precipitating causes or associated conditions, including childbirth, serious illness, including HIV infection, high fever, life-threatening trauma, major surgery, restrictive dieting and nutritional deficiencies, hypothyroidism, iron-deficiency anemia, medications, especially hormonal drugs, allergic contact dermatitis, the onset of androgenetic alopecia, and psychological stress . The shedding tends to occur diffusely throughout the scalp and may involve hair over the rest of the body.
Telogen hairs are recognizable by the club shape of their proximal end when visualized microscopically (club hairs). In conjunction with the history, physical examination of the scalp, and sometimes a trichogram (microscopic examination of shed, pulled, or plucked hairs), a diagnosis of telogen effluvium can often be made in the clinical setting. However, in difficult cases in which the differential diagnosis includes androgenetic alopecia and diffuse alopecia areata, a biopsy may be done.
|
|
Chronic telogen effluvium was a concept put forth by Whiting in 1996 after studying 355 patients with the disorder . Patients are usually middle-aged women 30 to 60 years of age with variable shedding that persists for years. Because hairs are replaced as fast as they are shed, patients do not become bald. An obvious cause is not
|
|
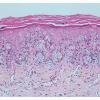
In late disease, permanent loss of terminal follicles occurs, with replacement of follicular tracts by scar tissue . These "follicular scars" resemble columns of fibrous tissue; interfollicular areas are uninvolved. Because vellus hairs are not sufficiently large to be included in the method of styling and be affected by tractional forces, these hairs are preserved, and this is reflected in a normal absolute number of vellus follicles, often
|
|