|
Scleredema, occasionally called scleredema adultorum even though it may occur in children and infants, is characterized by diffuse, nonpitting swelling and induration of the skin . Three groups can be recognized : one with abrupt onset, one with insidious onset, and one preceded by diabetes. In the first group, the scleredema starts abruptly during or within a few weeks after an upper respiratory tract infection. The
|
|
skin lesions may clear within a few months, or the disease may take a prolonged course. In the second group, the scleredema starts insidiously, for no apparent reason; spreads gradually; and takes a chronic course. The disease in the third group is preceded by diabetes for years, starts insidiously, and persists indefinitely. Usually, the scleredema starts on the face and extends to the neck and upper trunk. Unlike scleroderma, the hands and feet are always spared. In about 75% of patients, complete resolution takes place within a few months; in the remaining 25%, the disease may persist for as long as 40 years . Although visceral lesions may occur, death from scleredema is rare.
|
|
Diabetes is commonly associated with persistent scleredema and in most of these instances is quite resistant to antidiabetic therapy . It has been suggested that the association of persistent scleredema with maturity-onset diabetes be recognized as a special form of scleredema .
Histopathology
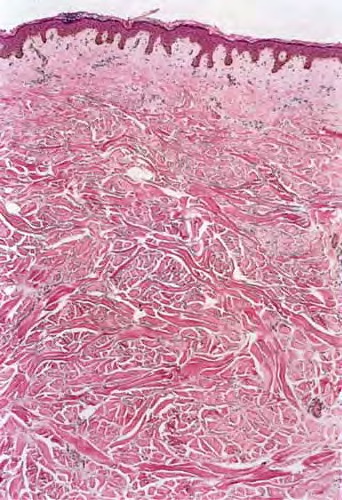
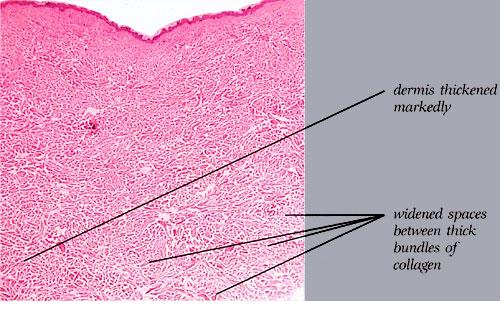
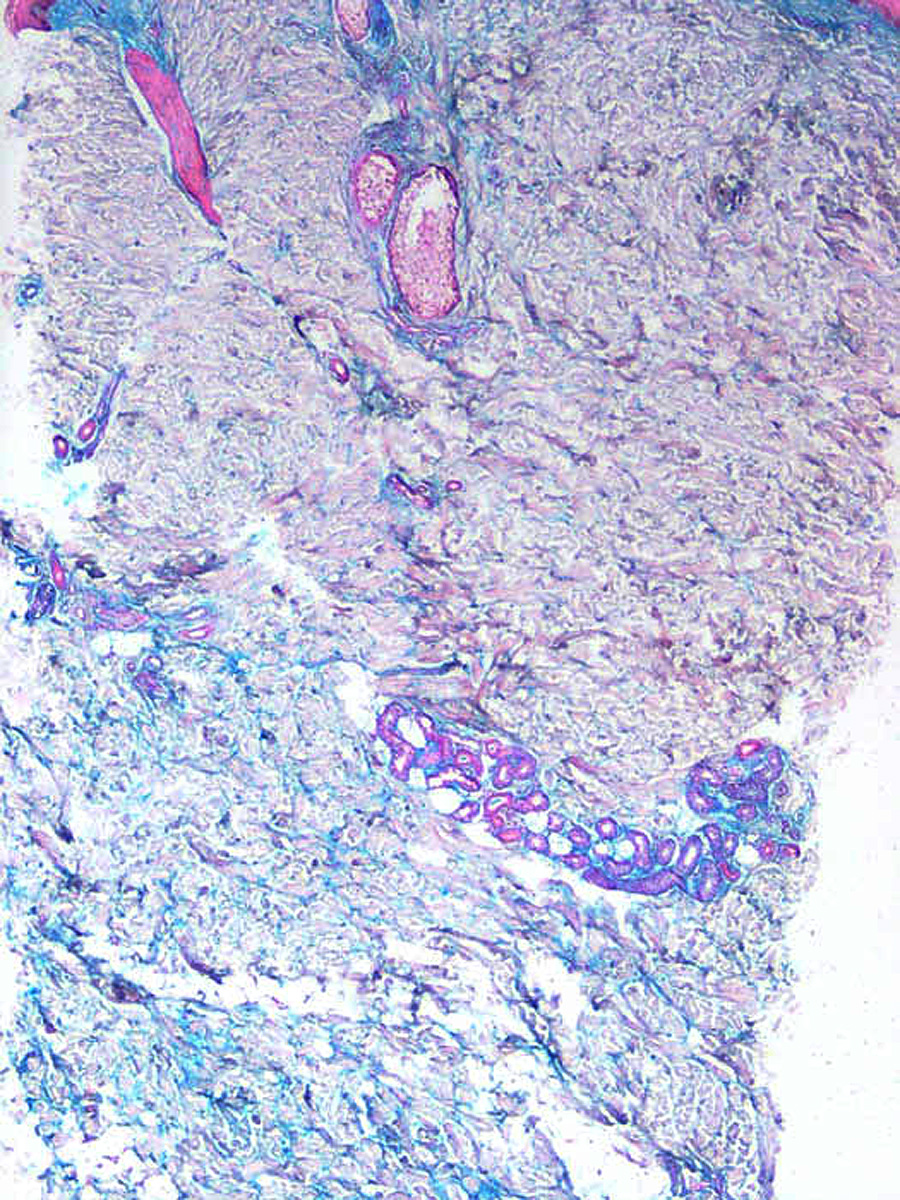
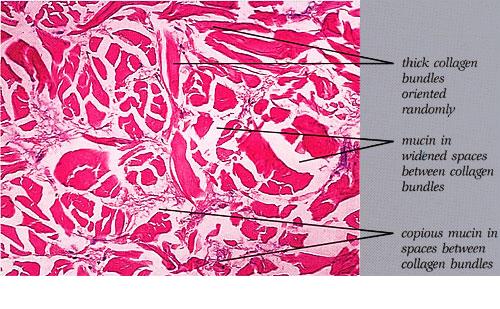
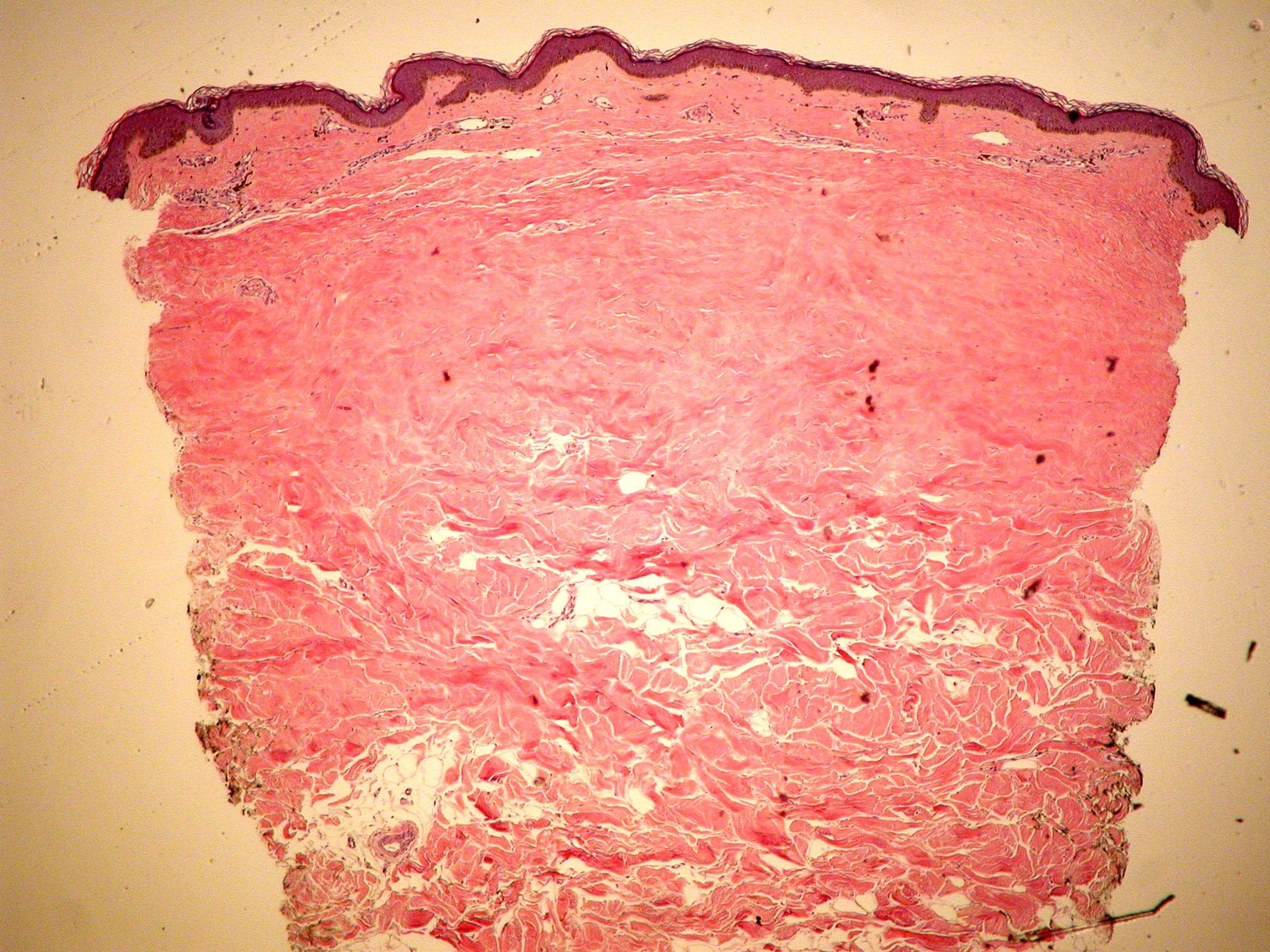
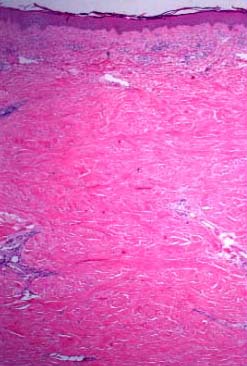
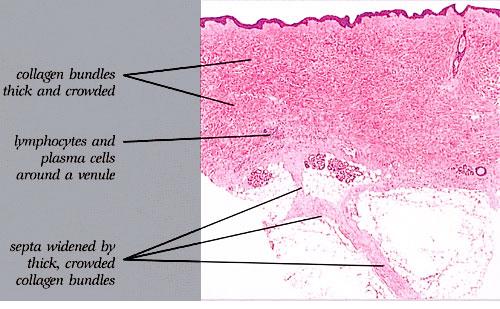
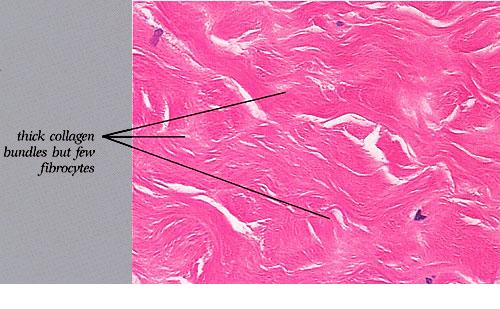
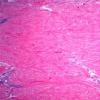
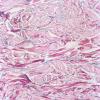
The dermis in scleredema is about three times thicker than normal . The collagen bundles are thickened and separated by clear spaces, causing "fenestration" of the collagen. The secretory coils of the sweat glands, surrounded by fat tissue, are located in the upper dermis or mid dermis rather than, as normally, in the lower dermis or at the junction of the dermis and the subcutaneous fat. Because the distance between the epidermis and the sweat glands is unchanged, it can be concluded that much of the subcutaneous fat in scleredema has been replaced by dense collagenous bundles . No increase in the number of fibroblasts is noted in association with the hyperplasia of the collagen; in fact, their number may be strikingly decreased .
|
|
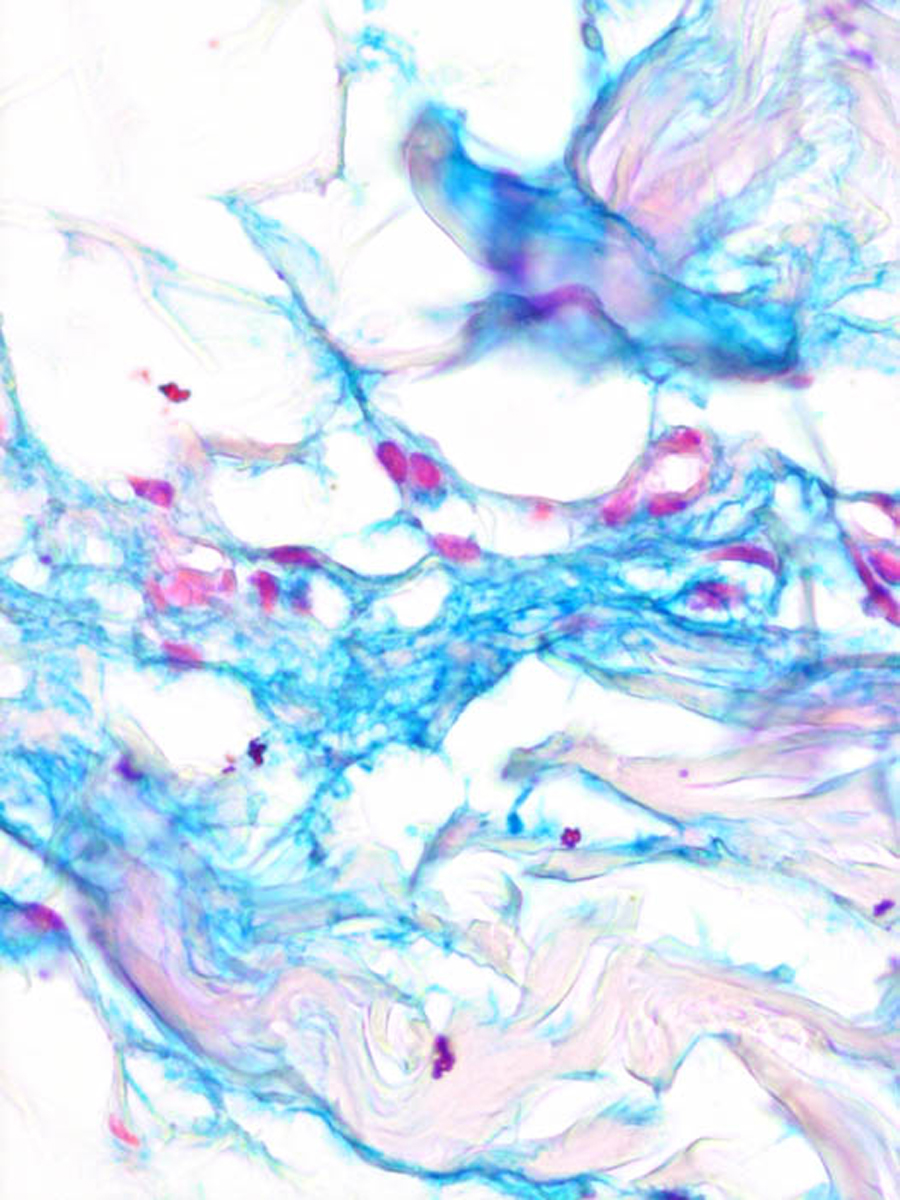
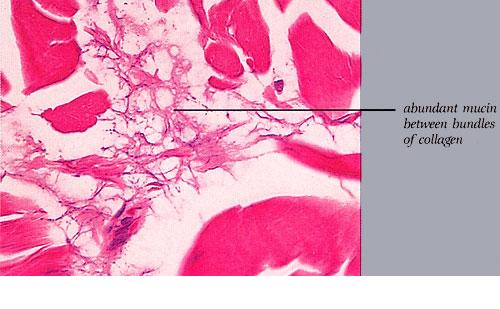
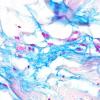
In many instances, especially in early cases, histochemical staining reveals the presence of hyaluronic acid between the bundles of collagen, particularly in the areas of fenestration. Staining with toluidine blue usually reveals metachromasia, which is most evident at pH 7.0, weaker at pH 5.0, and absent at pH 1.5, indicating the presence of only nonsulfated acid mucopolysaccharides . Although the hyaluronic acid is usually present throughout the dermis, it may be present only in the deeper portion of the dermis .
|
|
In some instances, staining with toluidine blue at pH 7.0 is more intense if unfixed cryostat sections are used in place offormalin-fixed material . In some cases, even frozen sections have failed to stain with Alcian blue or toluidine blue . It may be postulated that in long-standing cases in which the disease has reached a steady stage of collagen turnover, staining for hyaluronic acid may give negative results . In cases of scleredema in which formaldehyde-fixed specimens fail to show acid mucopolysaccharides, they may show them on fixation in 0.05% cetylpyridinium chloride solution and staining with Alcian blue at pH 2.5 . It has been stated that fixation with 1 % cetylpyridinium chloride solution in standard formalin fixative combined with colloidal iron staining gives the best results .
|
|
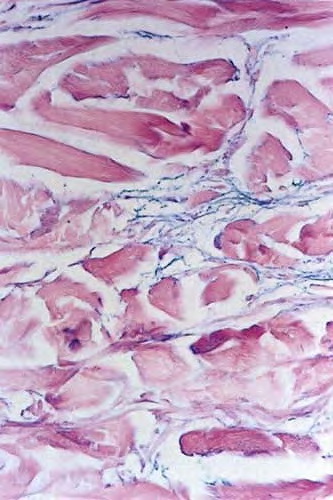
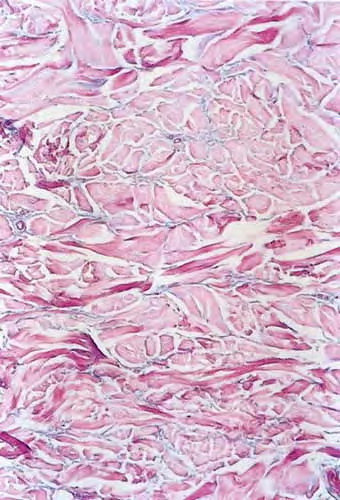
Systemic Lesions. Occasionally, the tongue and some skeletal muscles are involved, and on histologic examination, the muscle bundles show edema and loss of striation . In a few reported cases, pleural and pericardial effusions were present . In one case, the disease terminated in death, and autopsy revealed diffuse edema of the heart, liver, and spleen in addition to pleural and pericardial effusions .
|
|
Pathogenesis. In many patients with long-standing scleredema, a monoclonal gammopathy is found in the serum. Usually, the paraprotein is either IgG kappa or IgG lambda . In other cases, it has been IgA kappa, IgA lambda, or IgM lambda . There can be coexistence of scleredema with multiple myeloma . No immunoglobulin deposits have been found in involved skin sites . A marked increase in type 1 collagen gene expression occurs in scleroderma, leading to increased collagen synthesis .
|
|
Differential Diagnosis. It can be difficult to differentiate between end-stage scleroderma in which inflammation is no
|
|
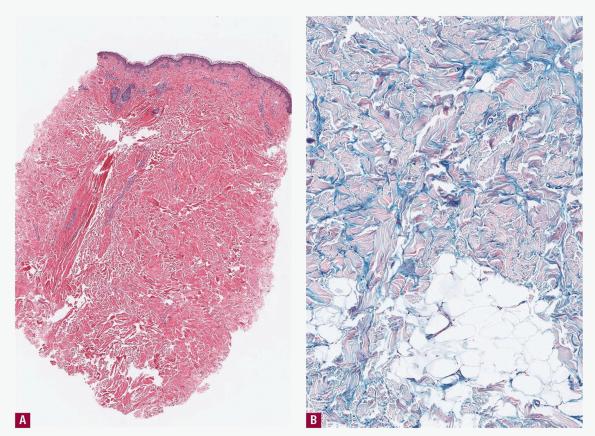
longer present and scleredema. As a rule, however, in scleroderma, the collagen in the reticular dermis and subcutaneous tissue appears homogenized and hyalinized and stains only lightly with eosin and with the Masson trichrome stain, but in scleredema, the collagen bundles are thickened without being hyalinized and stain normally with eosin and the trichrome stain . A marked increase in type 1 collagen gene expression occurs in scleroderma, leading to increased collagen synthesis
|
|