|
In this disorder, genetically abnormal elastic fibers with a tendency toward calcification occur in the skin and frequently also in the retina and within the walls of arteries, particularly the gastric mucosal arteries, coronary arteries, and large peripheral
|
|
arteries. The inheritance is usually autosomal recessive but is occasionally autosomal dominant. It seems that two recessive and two dominant forms exist. Struk predicted that allelic heterogeneity with different variants of a single disease gene residing on 16p13.1 accounts for both recessive and dominant forms of pseudoxanthoma elasticum, and subsequent work by Ringpfeil and Struk have documented that mutations in the ABC-C6 gene are responsible for cases of pseudoxanthoma elasticum . The classic disorder in this classification is recessive type 1. In the dominant type 1, the cutaneous and internal manifestations are more severe than in recessive type 1, whereas in dominant type 2 they are less severe. The very rare recessive type 2 shows only cutaneous involvement, which, however, is extensive . The accuracy of the Pope classification has been disputed, leading to a new classification .
|
|
The cutaneous lesions usually appear first in the second or third decade of life and are generally progressive in extent and severity. They consist of soft, yellowish, coalescing papules, and the affected skin appears loose and wrinkled. The sides of the neck, the axillae, and the groin are the most common sites of lesions . In the eyes, so-called angioid streaks of the fundi may cause progressive impairment of vision. Involvement of the arteries of the gastric mucosa may lead to gastric hemorrhage; involvement of coronary arteries may result in attacks of angina pectoris, although myocardial infarction is rare; and involvement of the large peripheral arteries may cause intermittent claudication . Radiologic examination in such cases reveals extensive calcification of the affected peripheral arteries .
|
|
In rare instances, the coexistence of pseudoxanthoma elasticum with elastosis perforans serpiginosa has been reported, with perforation and transepidermal elimination present only in the lesions of elastosis perforans serpiginosa (249). Calcific elastosis, which has been referred to also as perforating pseudo-xanthoma elasticum or localized acquired pseudoxanthoma elasticum, is not related to pseudoxanthoma elasticum. The absence of skin lesions should not be used to exclude pseudo-xanthoma elasticum in patients with an inherited predisposition and suspicious manifestations, such as angioid streaks or gastric bleeding. In these patients, biopsies of scars or of flexural skin may show the characteristic changes of pseudoxanthoma elasticum in the deep dermis .
|
|
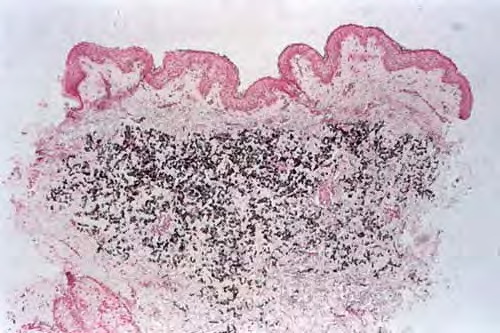
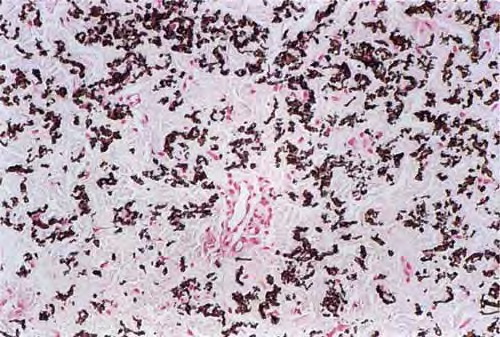
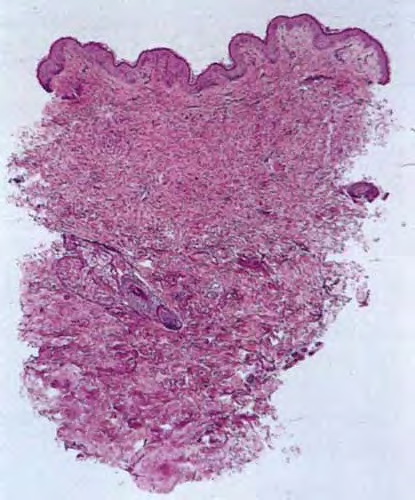
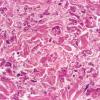
Histopathology.
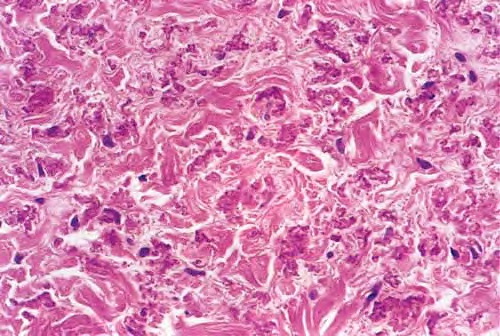
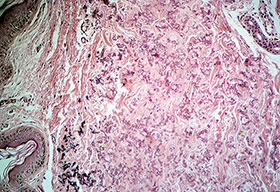
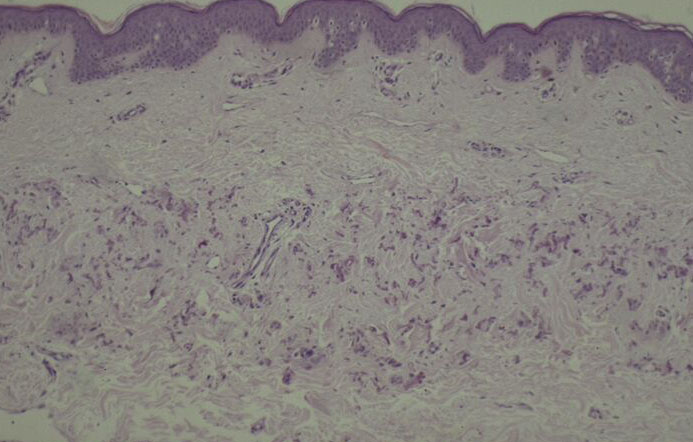
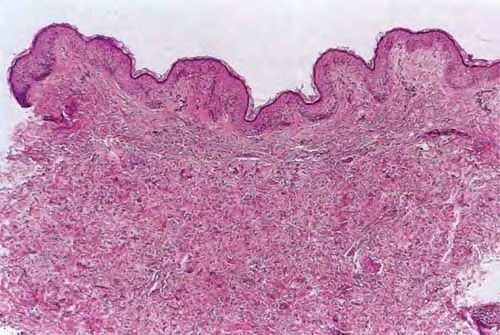
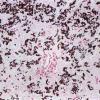
Histologic examination of the involved skin reveals considerable accumulations of swollen and irregularly clumped fibers staining like elastic fibers in the middle and lower thirds of the dermis; that is, they stain deeply black with orcein or Verhoetrs stain . Although normally elastic fibers do not stain with routine stains such as hematoxylin-eosin, the altered elastic fibers in pseudoxanthoma elasticum stain faintly basophilic because of their calcium imbibition. Staining for calcium with the von Kossa method also shows these fibers well.
|
|
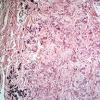
In the vicinity of the altered elastic fibers, there may be accumulations of a slightly basophilic mucoid material, which stains strongly positive with the colloidal iron reaction or with Alcian blue . The number of collagen bundles is reduced in such areas, and numerous reticulum fibers are seen on impregnation with silver . In some cases with pronounced elastic tissue calcification, a macrophage and giant cell reaction may be present .
|
|
The angioid streaks occur in Bruch's membrane, which is located between the retina and the choroid and possesses numerous elastic fibers in its outer portion, the lamina elastica. Calcification of these fibers causes fissures to form in the lamina elastica. These fissures result in repeated hemorrhages and exudates, which in turn cause degenerative changes in the retina consisting of scar formation and pigment shifting .
|
|
Gastric bleeding is the result of calcification of elastic fibers in the thin-walled arteries located immediately beneath the gastric mucosa. The internal elastic lamina is particularly affected. In muscular arteries, such as the coronary arteries and the large peripheral arteries, calcification begins in the intemal and external elastic laminae, leading to their fragmentation, and subsequently extends to the media and intima . Calcification of the elastic fibers in the endocardium is a common occurrence but is clinically silent .
|
|
Histogenesis. Electron microscopic examination shows that the calcification occurs in normal-appearing elastic fibers . In some patients, especially in young persons, only some of the elastic fibers in the lower dermis are calcified, and the calcification is variable in degree. However, in adult patients, most elastic fibers show considerable calcification and, as a result, degeneration. Early calcification of elastic fibers consists either of diffuse granular deposits throughout the elastic fiber or of dense aggregates that may be located in the center or near the margin of the fiber (EM 5). With progression of the calcification, the elastic fibers ultimately become fully calcified, showing marked swelling and bizarre distortions. In addition, heavy calcium deposits may be seen in the ground substance adjacent to elastic fibers and free in the ground substance. The presence of calcified material outside of elastic fibers can be explained by the disintegration of completely calcified elastic fibers .
|
|
Besides varying numbers of normal collagen fibrils, irregularly twisted collagen fibrils and granulofilamentous aggregates are present. It appears unlikely that the process of calcification begins in the granulofilamentous material, as maintained by some authors who regard this material as an abnormal precursor of elastic fibers . It is probable that this misinterpretation has resulted from the examination of advanced lesions containing disintegrated calcified elastic fibers within the granulofilamentous material . In favor of a primary location of the calcification within elastic fibers is the important observation that in decalcified sections of endocardial lesions, the internal structure of the calcified segments of elastic fibers is very similar to that of the adjacent noncalcified segments.
|
|
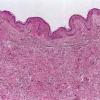
Differential Diagnosis. Solar elastosis, like pseudoxanthoma elasticum, shows abnormal elastic tissue. However, in solar elastosis, this material is located in the upper third of the dermis and is present as dense masses rather than as individual altered fibers. Furthermore, these dense masses always show negative staining for calcium. If associated with a perforation, calcific elastosis is easily distinguished from pseudoxanthoma elasticum. In the absence of a perforation, the two are indistinguishable, and clinical data are necessary for differentiation.
|
|