|
Polyarteritis nodosa = التهاب الشرايين العقد |
 |
|
Polyarteritis Nodosa
Clinical Presentation.
Systemic polyarteritis nodosa can affect the skin by several types of presentations. The affected arteries are deeply located, in the deep dermal vascular plexus at the
|
|
junction of dermis and subcutis or in the deep subcutis itself. A common clinical manifestation is a region of netlike erythema (livedo reticularis), with some tenderness to palpation. This livedo is fixed and not transient or altered by the temperature of the environment. To obtain a biopsy of the affected deep artery, it has been shown that the exact site and depth are important. The affected artery may lie deep beneath the center of the pale area, which is surrounded by a rim of redness due to vasodilation at the periphery of the ischemic region. Biopsies into those red netlike lines visible at the skin surface often miss or show very little of the affected artery. Systemic manifestations can be reflected in hypertension, proteinuria, elevated circulating immune complexes, decreased complement levels, deep muscle tendemess and pain, and cerebral infarcts. In Sneddon's syndrome, the combination of livedo reticularis and cerebral infarcts can be due to polyarteritis nodosa, hypercoagulable states, or lupus erythematosus. Cutaneous manifestations of polyarteritis nodosa are common in hepatitis C infection. Superficial biopsies may show only telangiectasia and extravasation of erythrocytes, or occasionally a mild leukocytoclastic vasculitis, probably depending on the sizes of the circulating immune complexes, and the degree of permeability of the endothelium. Some patients with histologically demonstrated polyarteritis nodosa on skin biopsy have a form of polyarteritis that tends to remain limited to the skin for prolonged time periods. Some cases have not shown involvement other than in the skin and subcutaneous tissue for as many as 15 years, which has given dermatologists the impression that there is a distinct entity of skin-limited polyarteritis nodosa, often named cutaneous polyarteritis nodosa. Follow-up studies of such patients have shown that despite being initially limited to the skin histologically and clinically, cutaneous polyarteritis nodosa may show signs of systemic disease at variable time periods after initial diagnosis in a considerable proportion of the patients. Hypertension, hematuria, testicular and muscle biopsies showing polyarteritis, and serum tests indicative of hepatitis B or C infection all point to systemic rather than localized cutaneous polyarteritis . Perhaps the exact nature and sizes of the circulating immune complexes could explain the overlapping features and why the disease manifestations are
|
|
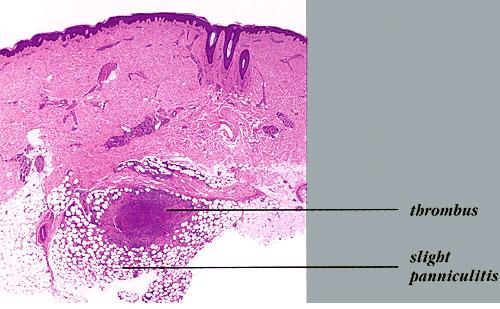
Differential Diagnosis. The distinction between polyarteritis and thrombophlebitis has been discussed previously in the section on thrombophlebitis (previous page). The distinction between systemic versus localized cutaneous polyarteritis depends heavily on the degree of investigation of the systemic factors, including the presence of proteinuria or hematuria (the glomeruli filter out circulating immune complexes). Elevations in muscle enzymes and muscle tenderness could lead to muscle biopsy as part of the investigation. Hypertension may also be a related systemic phenomenon. Investigation into the possible circulating viral antigens, such as hepatitis B or C, could also be revealing of systemic disease. It is most unlikely that arteritis will remain localized only to the skin when it is due to circulating immune complexes. Hypercoagulable states and lupus erythematosus need to be excluded.
|
|
limited to the skin for a long time in some patients. Polyarteritis nodosa can lead to deep ulceration of the skin into the subcutis. Some authors have analyzed the same information and have presented the entity of cutaneous polyarteritis as a special distinct condition by discounting the overlap with systemic disease and the importance of following the patients over time .
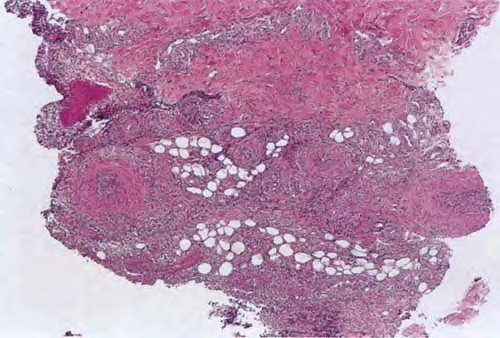
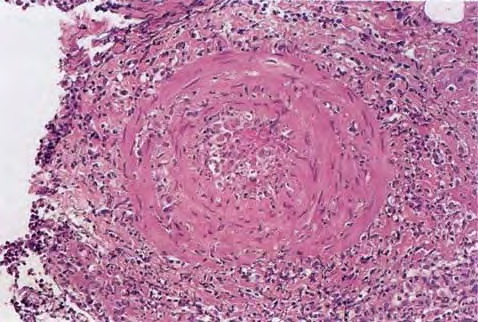
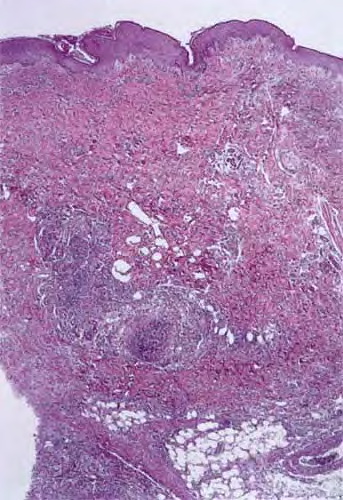
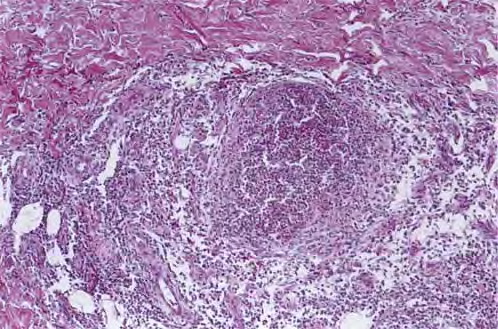
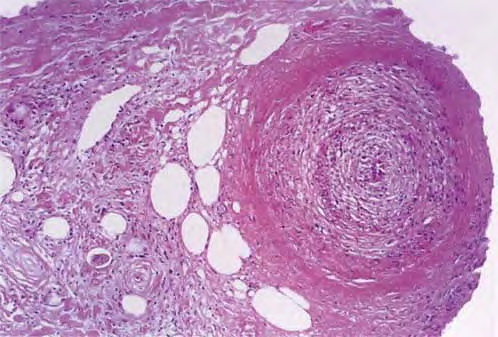
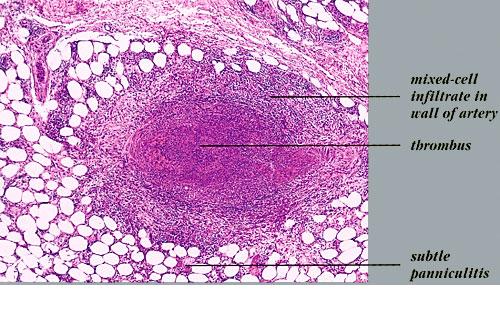
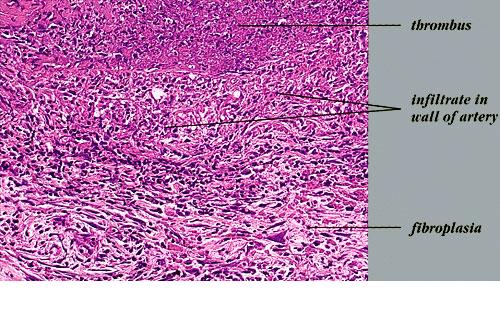
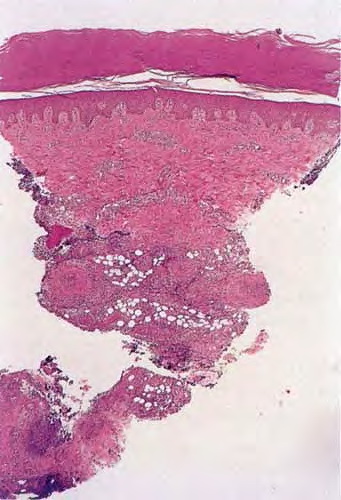
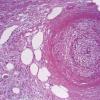
Histopathology.
The inflammatory infiltration into the walls of arteries and arterioles tends to be focal. Segments along the length of the artery are involved differently and may have only a portion of its cross-sectioned profile involved by the destructive inflammation . The focal areas have fibrin deposition in the vessel wall with necrosis of the intimal and medial portions of the vessel. Early lesions have mostly neutrophilic infiltration, with destruction of them to produce fragmented segments of the nuclei, nuclear dust. Later lesions have more lymphocytic infiltrate into the vessel as well as around it. Macrophage infiltration is also part of the process of resolution of the lesion. Immunofluorescence has shown immune complexes in the vessel walls (immunoglobulins G and M [lgG; IgM] and C3). The vascular destruction often does not completely occlude the lumen, which is in part a consequence of the tendency of dermatologists to biopsy early lesions rather than ulcerated ones. Some authors have stressed a difference in the localization of the lesions to the bifurcations of arteries in systemic polyarteritis and not in cutaneous polyarteritis . Such differences, if they are present, may be related to hydrostatic shear stress forces being greater at bifurcations and greater in patients with hypertension. Since the arteries tend to be in the deep dermal plexus and in the septa, the inflammatory process in the subcutis is classified as a septal panniculitis with vasculitis.
|
|