|
Poikiloderma Atrophicans Vasculare
Poikiloderma atrophicans vasculare may be seen in three different settings: (a) in association with three genodermatoses, (b) as an early stage of mycosis fungoides, and (c) in association with dermatomyositis and, less commonly, lupus erythematosus.
|
|
The three genodermatoses in which the cutaneous lesions have the appearance of poikiloderma atrophicans vasculare are (a) poikiloderma congenitale of Rothmund- Thomson (see Chapter 6), with the lesions of poikiloderma present largely on the face, hands, and feet, and occasionally also on the arms, legs, and buttocks; (b) Bloom's syndrome (see Chapter 6), with poikiloderma-like lesions on the face, hands, and forearms; and (c) dyskeratosis congenita (see Chapter 6), in which there may be extensive netlike pigmentation of the skin suggestive of poikiloderma atrophicans vasculare.
|
|
Poikiloderma-like lesions as features of early mycosis fungoides may be seen in one of two clinical forms: either as the large plaque type of parapsoriasis en plaques, also known as poikilodermatous parapsoriasis , or as parapsoriasis variegata, also called parakeratosis variegata, which, in its early state, shows papules arranged in a netlike pattern . Although these two types of parapsoriasis represent an early stage of mycosis fungoides, not all cases progress clinically into fully developed mycosis fungoides . Cases in which no progression toward mycosis fungoides is observed have been described also as idiopathic poikiloderma atrophicans vasculare .
|
|
The third group of diseases in which lesions of poikiloderma atrophicans vasculare occur are represented by dermatomyositis and SLE. Dermatomyositis is much more commonly seen as the primary disease than lupus erythematosus, and the association with dermatomyositis often is referred to as poikilodermatomyositis. In contrast to mycosis fungoides, in which poikilodermatous lesions are seen in the early stage, the lesions found in dermatomyositis and SLE generally represent a late stage.
|
|
Clinically, the term poikiloderma atrophicans vasculare is applied to lesions that, in the early stage, show erythema with slight, superficial scaling, a mottled pigmentation, and telangiectases. In the late stage the skin appears atrophic and the erythema is less pronounced than in the early stage, but the mottled pigmentation and the telangiectases are more pronounced. The clinical picture then resembles that of chronic radiodermatitis.
|
|
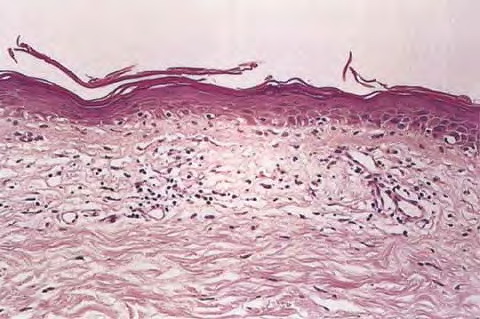
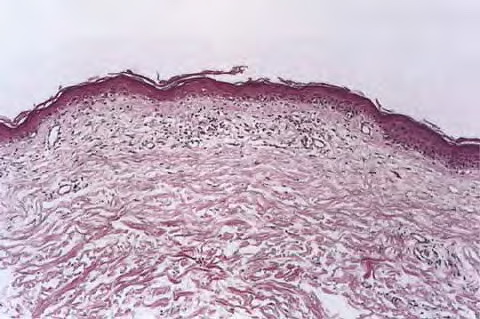
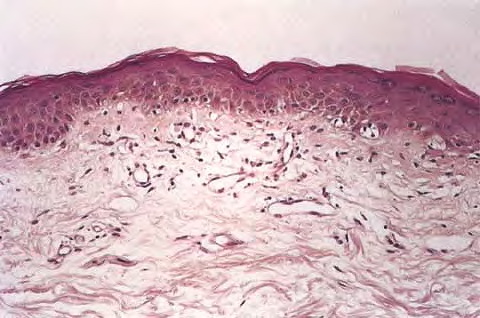
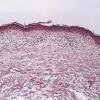
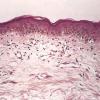
Histopathology.
In its early stage poikiloderma atrophicans vasculare, without respect to its cause, shows moderate thinning of the stratum malpighii, effacement of the rete ridges, and hydropic degeneration of the basal cells. In the upper dermis there is a bandlike infiltrate, which in places invades the epidermis. The infiltrate consists mainly of lymphoid cells, but it also contains a few histiocytes. Melanophages filled with melanin as a result of pigmentary incontinence are found in varying numbers within the infiltrate. In addition, there is edema in the upper dermis, and the superficial capillaries are often dilated. In the late stage the epidermis is apt to be markedly thinned and flattened, but the basal cells still show hydropic degeneration. Melanophages and edema of the upper dermis are still present, and telangiectasia may be pronounced.
|
|
The amount and type of dermal infiltrate vary with the underlying cause. In poikiloderma atrophicans vasculare associated with one of the genodermatoses the mononuclear infiltrate is mild and may be absent in the late stage . Similarly, in the late stage of poikiloderma seen in association with dermatomyositis or SLE there is only slight dermal inflammation . In contrast, the amount of inflammatory infiltrate seen in poikiloderma associated with early mycosis fungoides increases rather than decreases with time . In addition, cells with large, hyperchromatic nuclei, so-called mycosis cells, are likely to be present, and there is often marked epidermotropism of the infiltrate, which may result in Pautrier microabscesses. Cell-marker analysis of such cases has shown most cells to be T-helper/inducer (CD4+) lymphocytes that lack Leu-8 (CD?) and/or Leu-9 expression, as seen in cutaneous T-cell lymphoma .
|
|