|
Pigmented spindle cell melanocytic tumor = ورم الخلايا الميلانية المغزلية المصطبغ |
 |
 |
 |
|
Pigmented Spindle Cell Nevus
This tumor, first described by Richard Reed in 1973 , may be regarded as a variant of the Spitz nevus
or as a distinctive clinicopathologic entity . In our experience and that of others, most cases differ significantly from classical Spitz nevi, but some present with overlapping features, indicative of a close relationship between the two entities . Although this distinction has no clinical significance, in that each is a benign lesion, it is important to rule out melanoma, and this is facilitated by an understanding of the differences between these two common melanoma simulants.
|
|
The lesions are usually 3 to 6 mm in diameter, deeply pigmented, and either flat or slightly raised. Most patients are young adults, and the most common location is on the lower extremities. Pigmented spindle cell nevi are uncommon after the age of 35 years. A classic presentation is that of a newly evolved black plaque on the thigh of a young woman. Because of the heavy pigment and the history of sudden appearance, a diagnosis of melanoma is often suspected clinically. In contrast, Spitz nevi are usually submitted with a benign clinical diagnosis, such as an angioma or a dermal nevus. Like Spitz nevi, the lesions are generally stable after a relatively sudden appearance and a short-lived period of growth.
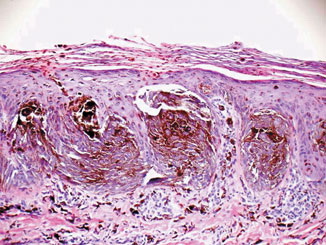
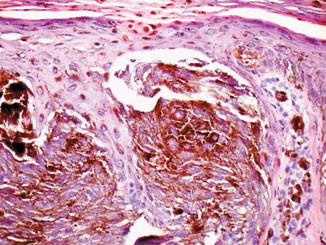
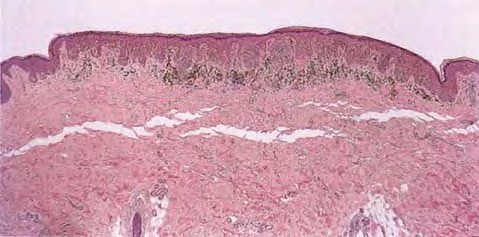
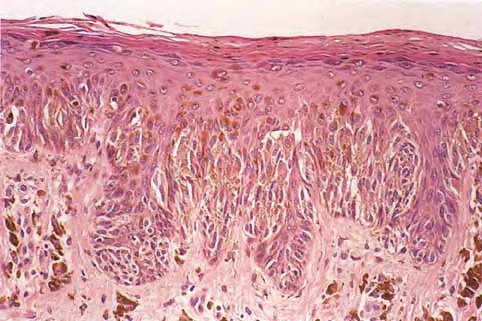
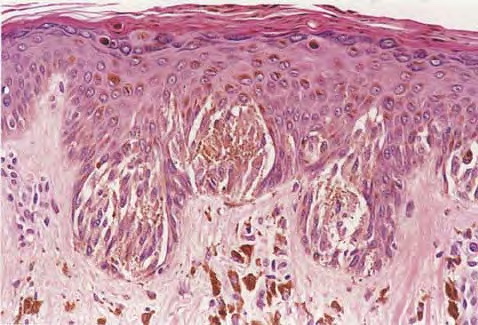
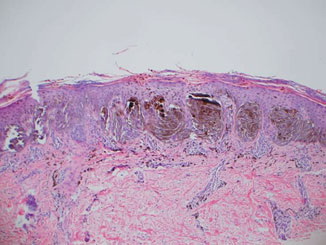
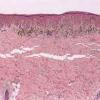
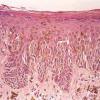
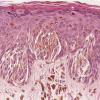
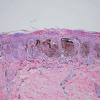
Histopathology.
The pigmented spindle cell nevus is characterized by its relatively small size and its symmetry and by a proliferation of uniform, narrow, elongated, spindle-shaped, often heavily pigmented melanocytes at the dermal-epidermal junction . The nests of spindle cells are vertically oriented and tend to blend with adjacent keratinocytes rather than forming clefts as in Spitz nevi. Eosinophilic globules (Kamino bodies) may be present . The tumor cells often form bundles that are separated by elongated rete ridges. In the papillary dermis, the nevus cells lie in compact clusters, pushing the connective tissue aside. Numerous melanophages are characteristically diffusely present within the underlying papillary dermis. Involvement of the reticular dermis, common in Spitz nevi, is unusual in pigmented spindle cell nevus. Some lesions show upward epidermal extension of junctional nests of melanocytes. Single-cell upward invasion of the epidermis in a pagetoid pattern may be present but is usually not prominent . Features that may lead to a diagnosis qualified as atypical pigmented spindle cell nevus include architectural abnormalities including poor circumscription and pagetoid melanocytosis, prominent cytologic atypia, or a prominent epithelioid cell component . There may also be considerable overlap with dysplastic nevi . The significance of these atypical variants appears to lie in their greater chance of being misdiagnosed as melanoma because all reports of pigmented spindle cell nevi emphasize their benign behavior after excision.
|
|
Differential Diagnosis.
The most important differential diagnosis is with melanoma of the superficial spreading type. In contrast to these melanomas, pigmented spindle cell nevi are smaller, symmetric, and show sharply demarcated lateral margins. The tumor cells appear strikingly uniform from side to side. If lesional cells of pigmented spindle cell nevi descend into the papillary dermis, they mature along nevus lines, in contrast to melanomas. Mitoses may be present in the epidermis in either lesion but are uncommon in the dermis in pigmented spindle cell nevi. Abnormal mitoses are exceedingly uncommon. Pagetoid melanocytosis is usually not prominent, and the spindle cell cytology differs from that of the epithelioid cells that predominate in most superficial spreading melanomas. Lentigo maligna melanomas may have spindle cells in their vertical-growthphase component, but the epidermal component is usually composed of smaller, nevoid, albeit atypical, cells. Some pigmented spindle cell nevi may present overlapping features with dysplastic nevi but can usually be distinguished on the basis of their irregularly thickened epidermis, their vertically oriented nests, and the uniformity of cell type, the absence of cytologic dysplasia, and the absence of typical stromal alterations (e.g., lamellar fibrosis). In cases of extreme doubt, we may classify the lesions as superficial atypical melanocytic proliferation of uncertain significance (SAMPUS) and provide a differential diagnosis of melanoma in situ or dysplastic nevus. In the former case, a reexcision procedure is recommended, whereas in the latter case we recommend assessment of melanoma risk factors and perhaps follow-up, especially if the patients have other clinically atypical nevi or a family or personal history of melanoma . Some rare examples of lesions with larger expansile intradermal nodules may be difficult to distinguish from melanoma, and a descriptive diagnosis may be appropriate
|
|
|
|
|