| Lupus vulgaris = الذأب الشائع |
|
|
Lupus Vulgaris
LV is an extremely chronic, progressive form of cutaneous tuberculosis occurring in individuals with moderate immunity and a high degree of tuberculin sensitivity.
Differential Diagnosis of Tuberculosis Verrucosa Cutis
Once common, LV has declined steadily in incidence. It has always been less common in the United States than in Europe. Females appear to be affected two to three times as often as males; all age groups are affected equally. PATHOGENESIS LV is a postprimary, paucibacillary form of tuberculosis caused by hematogenous, lymphatic, or contiguous spread from elsewhere in the body. Spontaneous involution may occur, and new lesions may arise within old scars. Complete healing rarely occurs without therapy. CLINICAL MANIFESTATIONS Lesions are usually solitary, but two or more sites may be involved simultaneously. In patients with active pulmonary tuberculosis, multiple foci may develop. In approximately 90 percent of patients, the head and neck are involved. LV usually starts on the nose, cheek, earlobe, or scalp and slowly extends onto adjacent regions. Other areas are rarely involved. The initial lesion is a brownish red, soft or friable macule or papule with a smooth or hyperkeratotic surface. On diascopy the infiltrate exhibits a typical apple jelly color. Progression is characterized by elevation, a deeper brownish color , and formation of a plaque . Involution in one area with expansion in another often results in a gyrate outline border. Ulceration may occur. Hypertrophic forms appear as a soft nodule or plaque with a hyperkeratotic surface (see eFig. 184-3.2 in on-line edition). Involvement of the nasal or auricular cartilage may result in extensive destruction and disfigurement . Atrophic scarring, with or without prior ulceration, is characteristic, as is recurrence within a scar. Fibrosis may be pronounced and mutilating. The mucosae may be primarily involved or become affected by the extension of skin lesions. Infection is manifest as small, soft, gray or pink papules, ulcers, or friable granulating masses. Dry rhinitis is often the only symptom of early nasal LV, but lesions may also destroy the cartilage of the nasal septum. Scarring of the soft palate and laryngeal stenosis also occur. After a transient impairment of immunity, particularly after measles (thus the term lupus postexanthematicus), multiple disseminated lesions may arise simultaneously in different regions of the body as a consequence of hematogenous spread from a latent tuberculous
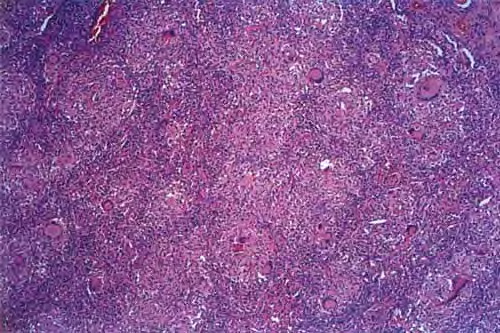
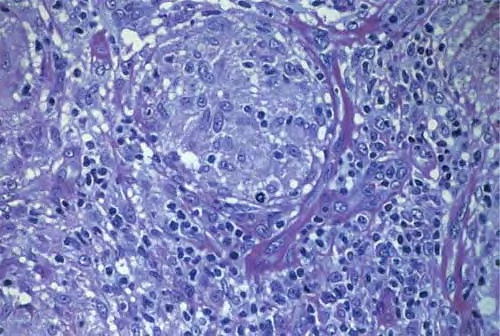
HISTOPATHOLOGY The most prominent histopathologic feature is the formation of typical tubercles. Secondary changes may be superimposed: epidermal thinning and atrophy or acanthosis with excessive hyperkeratosis or pseudoepitheliomatous hyperplasia. Acid-fast bacilli are usually not found. Non-specific inflammatory reactions may partially conceal the tuberculous structures. Old lesions are composed chiefly of epithelioid cells and may be impossible to distinguish from sarcoidal infiltrates . DIAGNOSIS Typical LV plaques may be recognized by the softness of the lesions, brownish red color, and slow evolution. The apple jelly nodules revealed by diascopy are highly characteristic; finding them may be decisive, especially in ulcerated, crusted, or hyperkeratotic lesions. The result of the tuberculin test is strongly positive except during the early phases of postexanthematic lupus. Bacterial culture results may be negative, in which case the clinical diagnosis can usually be supported by positive PCR results for M. tuberculosis . COURSE LV is a very long-term disorder and without therapy progresses over many years to functional impairment and disfiguration . Long-standing LV may lead to the development of carcinoma . Squamous cell carcinomas outnumber basal cell carcinomas by far, and the risk of metastases is high. In 40 percent of patients there is associated tuberculous lymphadenitis, and 10 percent to 20 percent have active pulmonary tuberculosis or tuberculosis of the bones and joints.11 Pulmonary tuberculosis is 4 to 10 times more frequent in patients with LV than in the general population.
TREATMENT OF CUTANEOUS TUBERCULOSIS In general, the management of cutaneous tuberculosis is similar to that of tuberculosis of other organs.Chemotherapy is usually the treatment of choice , but ancillary measures may be required. Vaccines against M. tuberculosis are under development.2 Although they are not yet established as a therapeutic option, cytokines such
Differential Diagnosis of Papulonecrotic Tuberculid
Special Considerations in Treating Tuberculosis of the Skin In contrast to systemic infection, for which triple-drug therapy is recommended, tuberculosis verrucosa cutis and localized forms of LV without evidence of associated internal tuberculosis may be treated with isoniazid alone for up to 12 months. Total doses of 80 to 140 g may be required. Because viable mycobacteria have been found in clinically healed lesions, treatment should be continued for at least 2 months after complete involution of the lesions. Surgical intervention is quite helpful in scrofuloderma, because it reduces morbidity and shortens the required length of chemotherapy. Small lesions of LV or tuberculosis verrucosa cutis are also best excised, but tuberculostatics should be given concomitantly. Plastic surgery is important as a corrective measure in cases of long-standing LV with mutilation.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||