|
Lupus Erythematosus Panniculitis
Clinical Features. In patients with chronic cutaneous lupus erythematosus, the lesions can be deep and can involve the dermis and subcutis or just the panniculus alone . The patients can have either chronic discoid lupus erythematosus or systemic lupus erythematosus. In about two thirds to one half of patients with these uncommon lesions, there are firm, indurated subcutaneous nodules with no specific clinical changes in the overlying skin. Histology is more sensitive and detects changes of discoid lupus erythematosus in 67% of these patients .
|
|
The lesions are deep nodules and plaques that tend to involve the skin of the trunk and proximal extremities, particularly the lateral aspects of the upper arms, thighs, and buttocks. Symmetrical lesions on the anterior chest or upper arms can suggest a traumatic or factitial etiology, and indeed trauma may playa role in the localization of the lupus inflammation to these sites. Approximately 70% of these patients also have other lesions that are typical of discoid lupus erythematosus, and 50% have evidence of mild systemic lupus erythematosus . The lesions are painful and have a tendency to ulcerate and to heal leaving depressed scars. When the overlying skin is involved, there is loss of hair, erythema, poikiloderma, and epidermal atrophy. Some patients present with localized depressions without erythema, clinically resembling lipoatrophy . The term lupus profundus has been used both for lupus panniculitis and also for discoid lupus erythematosus lesions that involve the dermis and extend deeply into the subcutis. Over time, lesions that begin as pure panniculitis can develop dermal sclerosis and leave deep depressions in the skin surface.
|
|
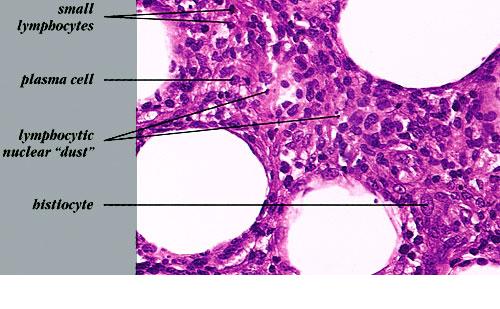
Histopathology.
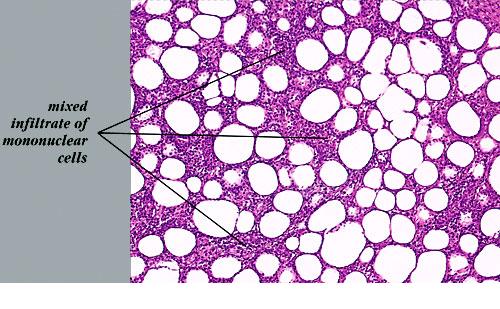
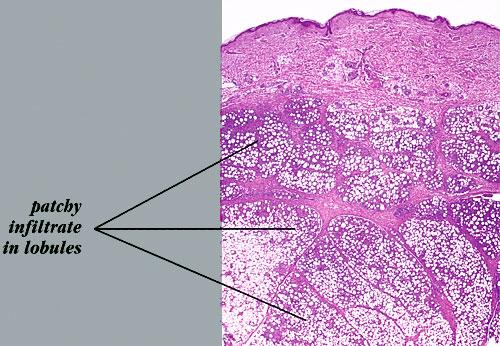
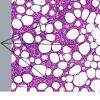
The histologic sections reveal a deep lymphocytic infiltration in the fat lobules and in the septa . Lymphoid aggregates, nodules, and germinal centers, also known as follicular centers, are common . The dermis can have just a superficial and deep perivascular lymphocytic infiltrate with plasma cells or can have all of the changes of lesions of discoid lupus erythematosus. A distinctive feature is the so-called "hyaline necrosis" of the fat, in which portions of the fat lobule have lost nuclear staining of the fat cells and have an accumulation of fibrin and other proteins in a homogeneous eosinophilic matrix between the residual fat cells and extracellular fat globules . Blood vessels are infiltrated by lymphoid cells and can have restriction of their lumen
|
|
diameter . Usually, there is mucinous edema of the septa and the overlying dermis . Calcification may be present in older lesions.
|
|
Pathogenesis. Approximately 50% of patients with lupus profundus have positive immunofluorescence findings at the dermal-epidermal junction and at hair follicle basement membranes. Usually there is granular deposition of IgM and C3 with linear deposition of fibrin. Granular deposits of IgG and immunoglobulin A (lgA) may be present also in active lupus cases. Many patients have similar deposits in deep dermal and subcutaneous blood vessel walls. Fibrin is distributed diffusely in the panniculus, both in the lobules and in the septa in areas with hyaline necrosis. It seems likely that trauma is involved in the localization of lesions, perhaps through increased vascular permeability and leakage of circulating antinuclear antibodies or immune complexes into the fat lobules. A few patients with lupus panniculitis have a partial genetic deficiency of C2 and C4 (75). A lupus-like syndrome has been reported in approximately one third of patients with C2 deficiency (76,77). In patients with complement at the dermal-epidermal junction, deposition of the so-called membrane-attack complex, composed of C5b-9, can be demonstrated as well.
|
|
Differential Diagnosis. Patients with lupus panniculitis have been given a clinical diagnosis of Weber-Christian disease in the past. The overlap in appearances may prevent any distinction between these two diseases by
routine histology. However, Weber-Christian disease can be sharply localized just to the fat lobules; in contrast, lupus panniculitis causes mucinous edema (detectable with Alcian blue stains) and inflammation around the blood vessels of the dermis and subcutis. Immunofluorescence and serologic studies allow a positive diagnosis of lupus erythematosus in many instances.
|
|
A particularly troublesome differential diagnosis is between lupus panniculitis and subcutaneous T-cell lymphoma . Although each of these two entities may have dense lymphoid infiltrates in the fat, usually the lymphoma has cytologically atypical lymphocytes. However, some cases of subcutaneous T-cell lymphoma are composed of small cells that lack obvious cytologic atypia in routine sections. A mixed population of CD4+ and CD8-positive T cells may be found, making T-cell receptor gene rearrangement studies necessary for showing a significantly high level of clonality in the lymphoid infiltrate. After these studies, there remain a few indeterminate cases on a spectrum from lupus panniculitis to subcutaneous T-cell lymphoma because they have been classified as lupus panniculitis, responsive to chloroquine and/or prednisone therapy, but have some slightly atypical cells, with CD5 and CD7 diminution, and DNA analysis that is suggestive of the presence of some clonal
|
|
lymphocytes in the population . Subcutaneous panniculitic T-cell lymphoma of the alpha/beta subtype, without evidence of a hemophagocytic syndrome, has an excellent prognosis (i.e., an 82% 5-year survival), even with some patients having conservative treatment. In contrast, subcutaneous T-cell lymphoma of the gamma/delta subtype has a much worse prognosis (i.e., an 11 % 5-year survival), even with intensive chemotherapy. Also, the gamma/delta subtype often involves overlying skin, with ulceration, and multiple other organ systems. The gamma/delta subtype should instead be classified as "gamma/delta T-cell lymphoma," with specification of the degree of involvement of the skin, subcutis, and internal sites. A natural killer (NK)/T-celllymphoma (CD2+ CD3CD56+ EBV+) can also be in the differential diagnosis .
Erythema induratum, like lupus panniculitis, also shows hyaline necrosis and vasculitis but has more granulomatous inflammation than in most cases of lupus panniculitis. Erythema induratum lacks the mucinous edema of the dermis.
|
|