|
Linear IGA Dermatosis = الجلاد الخطي IGA |
 |
 |
 |
|
Linear IgA Dermatosis
A group of bullous disorders mediated by IgA antibodies with differing specificities for epidermal basement membrane zone antigens has been labeled as LAD. The first and second relatively definitive clinical phenotypes are based on patient age and clinical features-adult LAD and childhood LAD (chronic benign bullous dermatosis of childhood). They differ slightly in their clinical presentations but have identical immunopathologic features. Third, a clinical phenotype similar to cicatricial pemphigoid has been described. Fourth, a subset of patients has been described with drug-induced LAD. On the basis of immunoelectron microscopic localization of the IgA deposition, there are at least two distinct types of LAD: a lamina lucida type and a sublamina densa type. Some of the sublamina densa types of LAD are best classified as IgA EBA.
|
|
Adult Type
Vesicles and bullae usually develop in patients >40 years of age, with a slight female predilection. The lesions are less symmetrical and less pruritic than those in dermatitis herpetiformis but may be distributed in similar locations. Ocular and oral lesions may be present in up to 50% of cases. Plantar and palmar bullae may develop in contrast to dermatitis herpetiform is. Cutaneous lesions in LAD are heterogeneous and may mimic other bullous diseases. LAD has been associated with an increased risk of lymphoma (119). Ulcerative colitis has been correlated with LAD in various studies, one of which found ulcerative colitis in 7.1 % of LAD patients (120). A rare association with SLE has been reported .
|
|
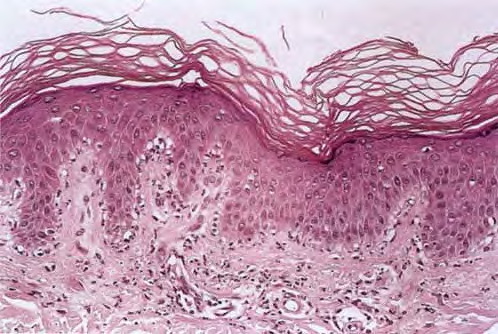
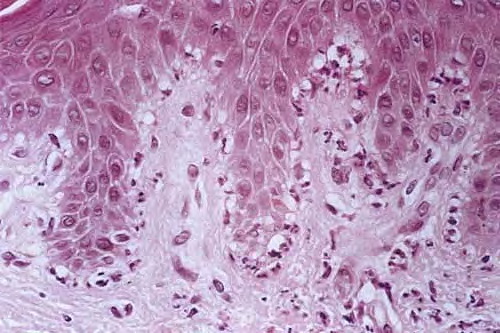
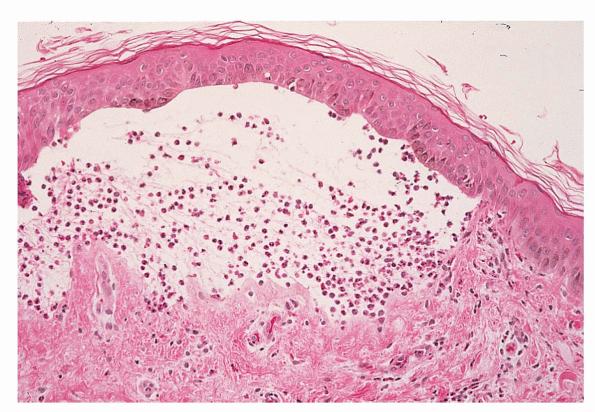
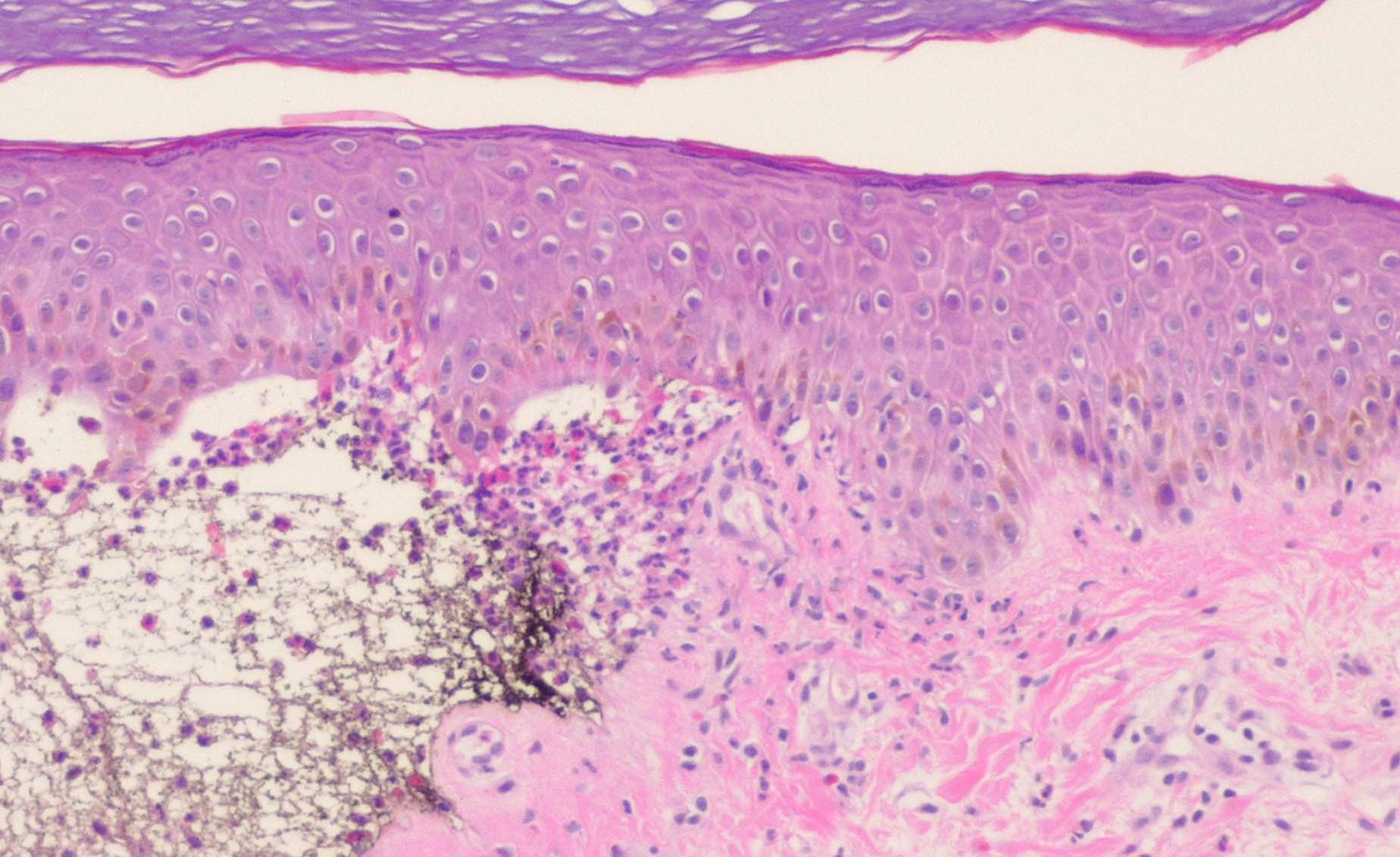
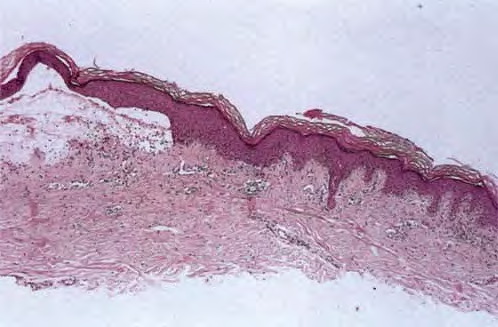
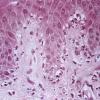
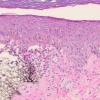
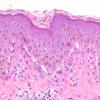
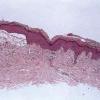
Histopathology.
The features are similar, if not identical, to dermatitis herpetiformis . According to some, there is less tendency for papillary microabscess formation and greater tendency for uniform neutrophil infiltration along the entire dermal-epidermal junction and rete in inflamed skin. Rarely, a principally lymphocytic infiltrate may be observed, sometimes with numerous neutrophils .
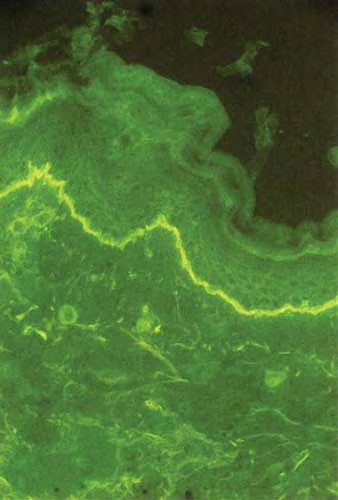
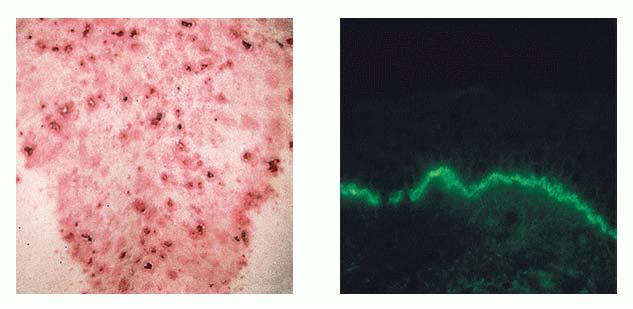
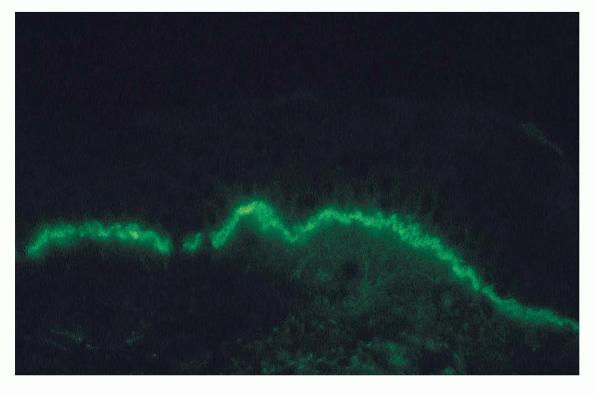
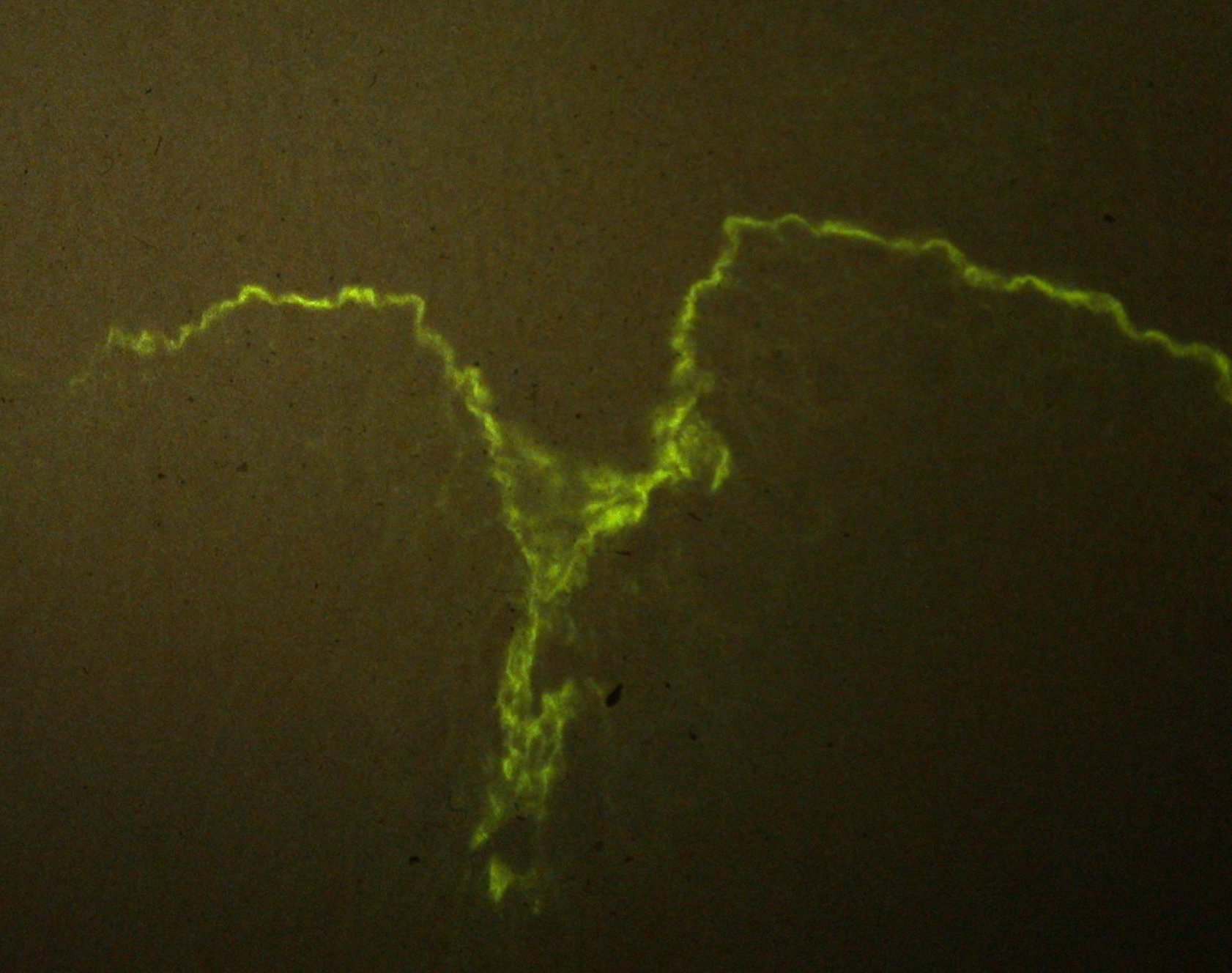
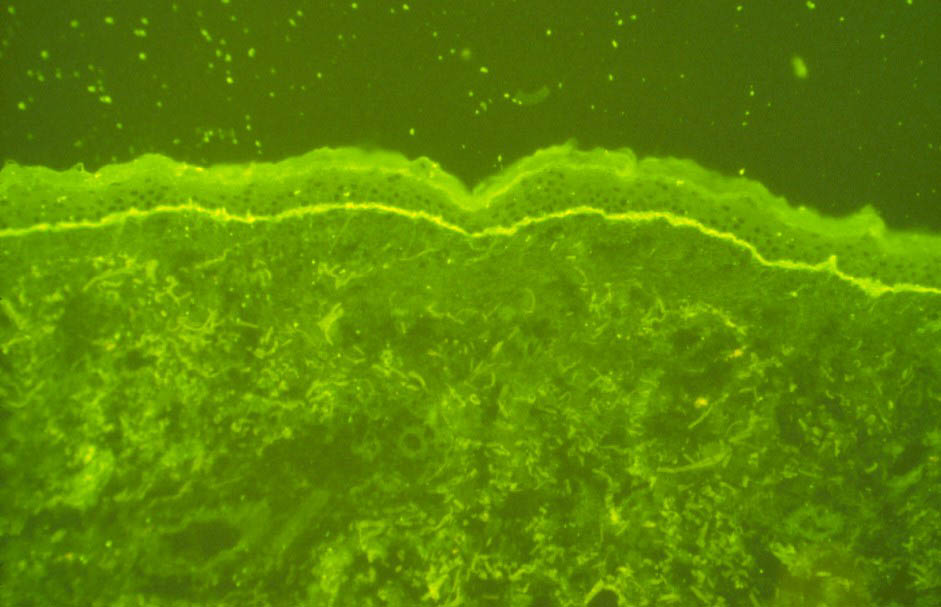
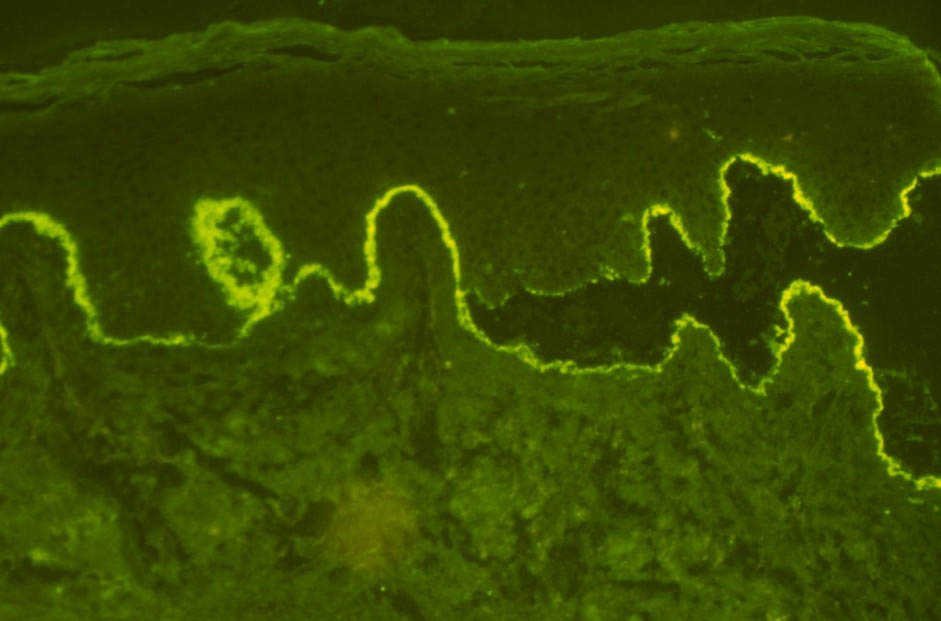
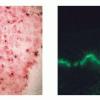
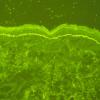
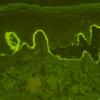
IF Testing. As this test defines the disease, DIF reveals linear IgA along the basement membrane zone in perilesional skin in 100% of cases (Fig. 9-23C). In the lamina lucida type of LAD, IgA antibodies bind to the epidermal side of salt-split skin, whereas in the sublamina densa type, such as IgA-mediated EBA, IgA antibodies bind to the dermal side of salt-split skin .
|
|
In the vast majority of cases, IgA 1, but rarely IgA2, is present. When IgG and IgA are present, some detailed immunologic study may be needed to allow differential diagnosis with bullous pemphigoid . It has been suggested that if the IgA deposits are more intense than the IgG deposits and C3 deposition is strong, then LAD is the best diagnosis. However, it is best considered a distinct disorder labeled as linear IgAllgG dermatosis until more data are available. One patient presented with linearly deposited IgG initially and only subsequently developed linear IgA deposits. Low titers of circulating anti-squamous basement membrane zone IgA have been identified in only 20% to 30% of cases . Another study, however, has noted such antibodies in up to 75% of patients.
Pathogenesis. In the lamina lucida type of LAD, the antigens against which the IgA is directed include a 97-kD and a 120-kD protein that may be found in epidermal and dermal extracts . Both of them are part of the cleaved ectodomain of the 180-kD bullous pemphigoid antigen (BPAg2). In the sublamina densa type, the antigen in many instances is unknown. In some cases, the antigen is
|
|
type VII collagen, specifically the NC-1 domain, which is the immunodominant epitope for EBA . The events of the inflammatory cascade in IgA-mediated diseases are not well understood.
|
|
Ultrastructural Study. The antibodies are deposited principally within the lamina lucida and less commonly beneath the lamina densa (lgA-mediated EBA).
|
|
Drug-associated Linear IgA Dermatosis
It is important to note that it is not infrequent for adult-type LAD to be associated with drug therapy. Vancomycin, lithium, diclofenac, captopril, cefamandole, and somatostatin have been associated with such presentations . Histologically, the changes are identical to idiopathic LAD in most cases. In some cases, there is an associated Iymphoeosinophilic infiltrate in combination with the interface neutrophilic infiltration.
|
|
Childhood Type
Originally known as chronic bullous dermatosis of childhood, this disorder presents in prepubertal, often preschool, children and rarely in infancy. Vesicles or bullae develop on an erythematous or normal base, occasionally giving rise to a so-called "string of pearls," a characteristic lesion in which peripheral vesicles develop on a polycyclic plaque . They involve the buttocks, lower abdomen, and genitalia and characteristically have a perioral distribution on the face. Oral lesions may occur. The disorder usually remits by 6 to 8 years of age, but 12% in one series experienced persistent disease.
|
|
Histopathology. The features are similar to those of the adult-type disease. Some cases, however, resemble bullous pemphigoid because of the presence of eosinophils.
|
|
IF Testing. DIF testing reveals linearly deposited IgA in virtually 100% of cases. At this time, the targeted antigens are thought to be identical to those noted in the adult-type disease. The sublamina densa type is uncommon in children (.
|
|
|
|
|