|
Lichen Sclerosus ET Atrophicus
Lichen sclerosus (LS) encompasses the disorders known as lichen sclerosus et atrophicus, balanitis xerotica oblitera ns (LS of the male glans and prepuce), and kraurosis vulvae (LS of the female labia majora, labia minora, perineum, and perianal region) . Lichen sclerosus is an inflammatory disorder of unknown etiology that affects patients 6 months of age to late adulthood. In both male and female patients genital involvement is the most frequent, and often the only, site of involvement. Extragenital lesions may occur with or without coexisting genital lesions.
|
|
Lesions of LS are characterized by white polygonal papules that coalesce to form plaques. Comedo-like plugs on the surface of the plaque correspond to dilated appendageal ostia. The plugs may disappear as the lesion ages, leaving a smooth, porcelain-white plaque. Solitary or generalized lesions may become bullous and hemorrhagic.
|
|
In male patients, involvement of the glans and prepuce often results in phimosis. Although the literature is dominated by reports of LS in incompletely or uncircumcised men , occurrences in circumcised men are reported as well . Neoplasms have been infrequently documented in association with LS; however, a causeand-effect relationship has not been established .
|
|
In female patients, contiguous involvement of the labial, perineal, and anal areas has been described clinically as "figure 8"
|
|
or "keyhole" lesions (165). Many cases of childhood LS in girls resolve by menarche (166). If lesions persist, atrophy of the labia and narrowing of the vaginal orifice may ensue. In contrast to lichen sclerosus et atrophicus of the skin, which rarely itches, there is often severe pruritus in the vulvar region.
|
|
The premalignant potential in LS has been debated extensively and remains ill defined. The most recent large population-based study detected a small increased risk of squamous cell carcinoma in patients with LS. Because neoplasms have arisen in areas adjacent to lesions of LS, long-term follow-up of patients with lichen sclerosus et atrophicus of the vulva is advisable.
|
|
Of interest, lesions of LS may koebnerize (be provoked by trauma) as well as coexist with morphea (167, 168). In extensive cases of morphea, lichen sclerosus et atrophicus may become superimposed on some of the lesions. It is then best
|
|
recognized by finding pale superficial dermal collagen, as compared with hypocellular compacted deep dermal collagen, and the presence of follicular plugging . Cases of both extragenital and genital LS have also been reported in the setting of graft-versus-host disease .
|
|
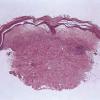
Histopathology.
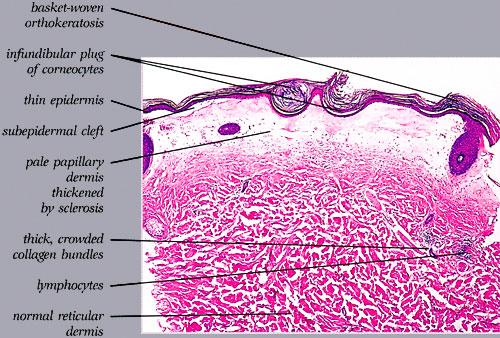
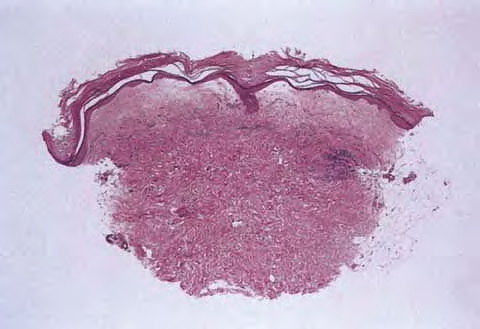
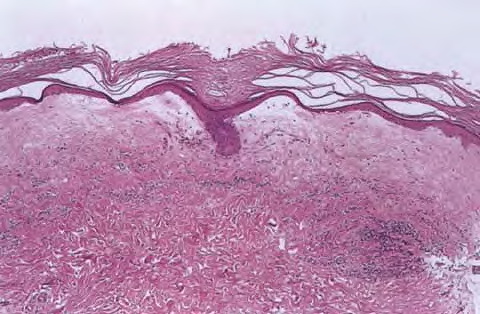
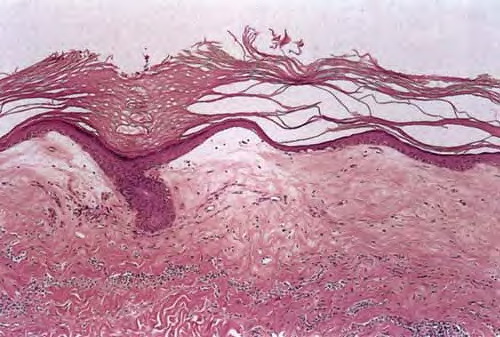
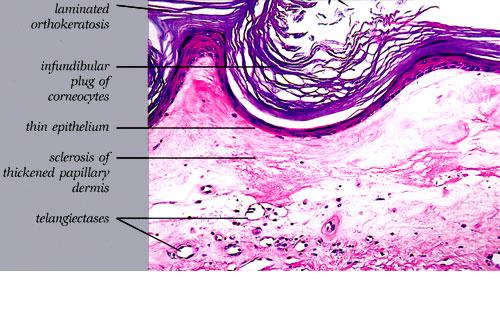
The salient histologic findings in cutaneous lesions of lichen sclerosus et atrophicus are (a) hyperkeratosis with follicular plugging, (b) atrophy of the stratum malpighii with hydropic degeneration of basal cells, (c) pronounced edema and homogenization of the collagen in the upper dermis, and (d) an inflammatory infiltrate in the mid-dermis.
|
|
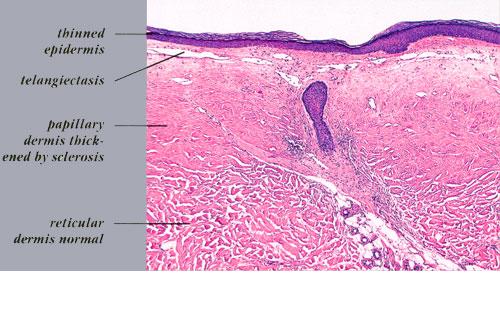
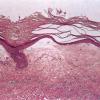
The hyperkeratosis is so marked that the horny layer is often thicker than the atrophic stratum malpighii, which may be reduced to a few layers of flattened cells . The cells of the basal layer show hydropic degeneration. The rete ridges often are completely absent, although they may persist in a few areas and show some irregular downward proliferation. In such proliferations, hydropic degeneration of the basal cells usually is pronounced.
|
|
Keratotic plugging of appendageal ostia is often associated with atrophy and disappearance of appendageal structures. Keratotic plugging is not apparent in mucosal lesions. In the latter areas, particularly the vulva, squamous hyperplasia adjacent to the atrophic epidermis can be found in about one third of patients with LS. There may be varying degrees of "dysplasia" consisting of disorderly arrangement of the cells and enlarged, hyperchromatic nuclei. Transition into carcinoma, however, is said to be rare .
|
|
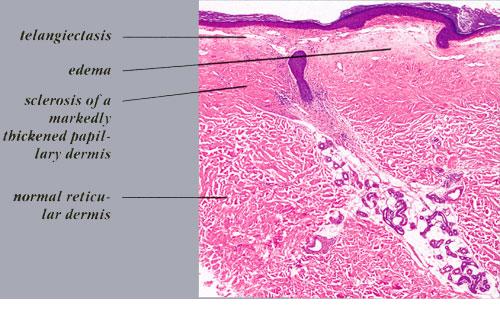
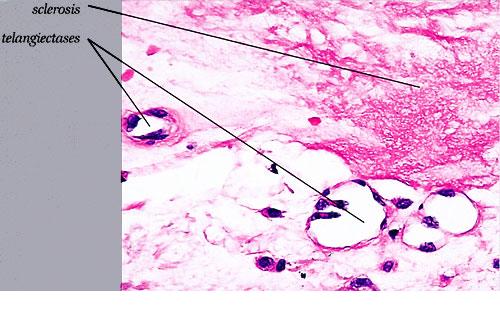
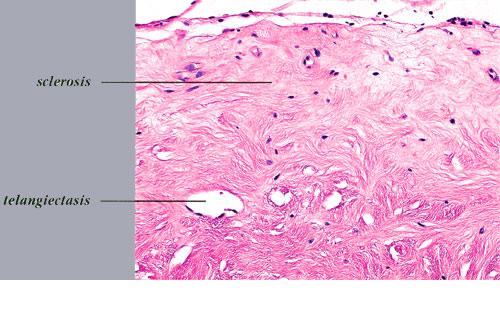
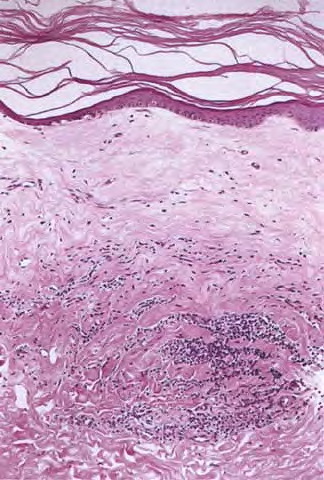
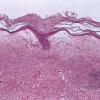
Beneath the epidermis is a broad zone of pronounced lymphedema . Within this zone, the collagenous fibers are swollen and homogeneous and contain only a few nuclei. They stain poorly with eosin and other connective tissue stains. The blood and lymph vessels are dilated, and there may be areas of hemorrhage. Elastic fibers are sparse and, in old lesions, are absent within the area of lymphedema . In areas of severe lymphedema, clinically visible bullae may form; they are found in subepidermal locations . Shrinkage within the area of lymphedema may occur during the process of dehydration of the specimen, resulting in the formation of pseudobullae, which often are located intradermally.
|
|
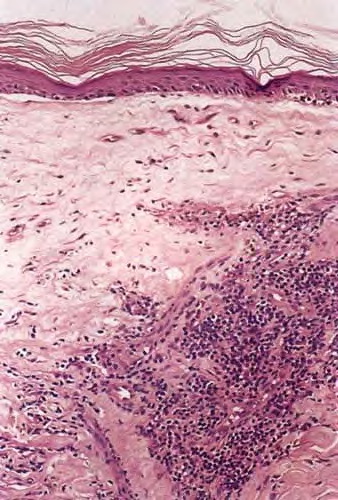
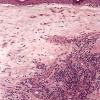
Except in lesions of long duration, an inflammatory infiltrate is present in the dermis. The younger the lesion, the more superficial is the location of the infiltrate. In very early lesions and at the periphery of somewhat older lesions, the infiltrate may be found in the uppermost dermis, in direct apposition to the basal layer. Soon, however, a narrow zone of edema and homogenization of the collagen displaces the inflammatory infiltrate farther down, so that, in well-developed lesions, the infiltrate is found in the mid-dermis. The infiltrate can be patchy, but it is often bandlike and composed of lymphoid cells admixed with plasma cells and histiocytes. In old lesions in which the infiltrate is slight or absent, the collagen bundles in the mid portion and lower dermis may appear swollen, homogeneous, and eosinophilic, thus appearing sclerotic (hence lichen sclerosus). Cases of overlap of morphea and LS may be seen and demonstrate the histologic changes of both disorders in their respective locations of the dermis .
|
|
Pathogenesis. Changes in the dermal matrix have been detected in LS. By electron microscopy, collagen fibrils often
|
|
lack cross-striation, and in cross sections they sometimes have the appearance of empty tubes, suggesting degeneration of collagen fibrils . In some areas, new immature collagen of reduced and variable diameter (40 to 80 nm) is seen . Ultrastructural studies also have shown degeneration of subepidermal elastin and increases in ground substance . The features all suggest an increased rate of matrix turnover or a dysregulated remodeling response. Studies examining the components of the dermal matrix have demonstrated increases in the matrix proteins tenascin and fibrinogen, which serve as scaffold proteins on which new collagen is deposited. Similar increases in tenascin and fibrinogen have been demonstrated in scleroderma and morphea, suggesting that this is may be a nonspecific change .
|
|
The frequent finding of human papillomavirus alterations in lesions of LS have lead some to consider LS an aberrant immune response to persistent antigenic stimulus. This notion is supported by the presence of LS
|
|
changes in cases of other
|
|
chronic vulvar dermatitides. It has been hypothesized that persistent antigen may lead to the presence of CD8/CD57-positive T cells, which may playa role in tissue remodeling and fibrosis though cytokine elaboration .
|
|
In the epidermis, intercellular edema separates epidermal cells that show degenerative changes. There is nearly a complete absence of melanosomes within the keratinocytes. Immunoperoxidase and Fontana-Mason stains of melanocytes have shown there is both a loss of melanocytes and decreased transfer of melanosomes to keratinocytes .
|
|
Differential Diagnosis.
Very early lesions may resemble lichen planus because of the apposition of the inflammatory infiltrate to the basal layer. However, the basal cells are not replaced by flattened squamous cells as in lichen planus but appear hydropic, and a subepidermal zone of edema usually has already begun to form in some areas in lichen sclerosus et atrophicus.
|
|
Old lesions of lichen sclerosus et atrophicus with thickening and eosinophilia of the collagen bundles in the midportion and lower dermis and only a slight inflammatory infiltrate may resemble morphea. Nevertheless, the epidermis in morphea, although it may be thin, shows neither hydropic degeneration of the basal cells nor follicular plugging, and the upper dermis in morphea has elastic fibers and shows no zone of edema . Still, in lesions in which lichen sclerosus et atrophicus develops either secondarily to morphea or simultaneously with it, there are, in addition to the epidermal and subepidermal changes of lichen sclerosus et atrophicus, changes indicative of morphea in the lower dermis and in the subcutaneous fat. A definite diagnosis of both lichen sclerosus et atrophicus and morphea in the same lesion can be made only if the newly formed collagen extends into the subcutaneous fat and consists offaintly staining, homogeneous collagen .
|
|