| Kimura's disease =داء كيمورا |
|
|
KIMURA DISEASE AND
ANGIOLYMPHOID
HYPERPLASIA WITH
EOSINOPHILIA
Epidemiology
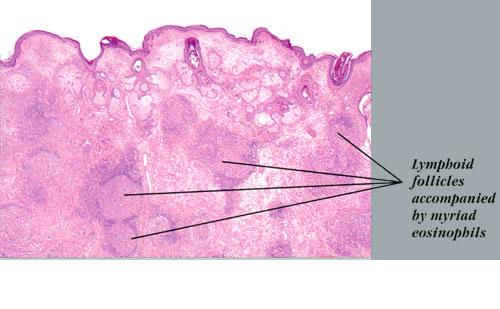
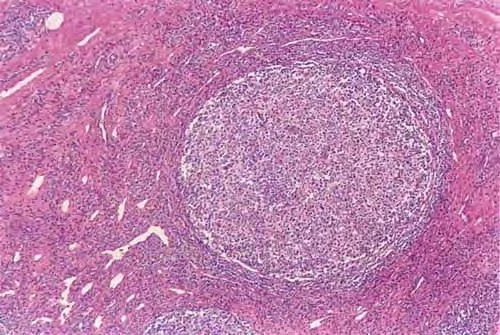
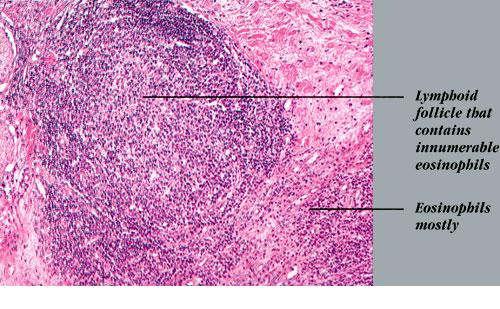
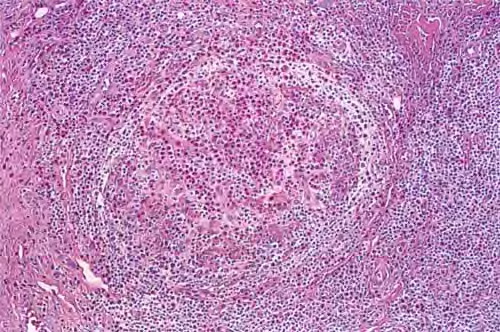
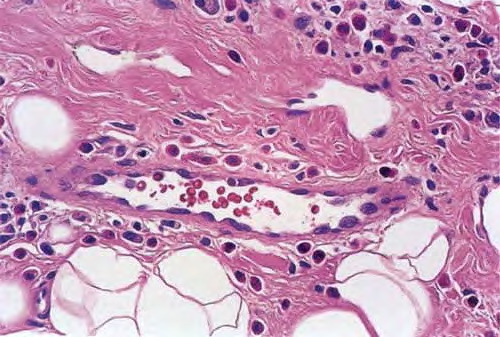
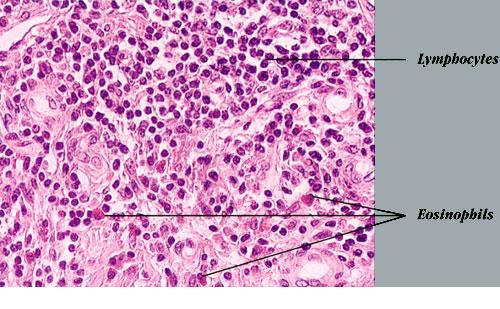
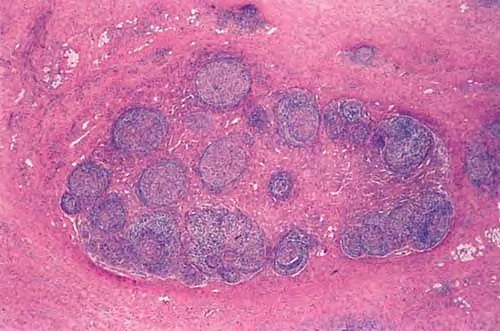
The skin lesions of Kimura disease and angiolymphoid hyperplasia with eosinophilia (AHLE) most commonly affect young to middle-aged adults. Kimura disease is more common in Asian men, whereas AHLE is more common in women. Etiology and Pathogenesis It is possible that Kimura disease represents a florid, subcutaneously deep-seated form of the same basic pathogenetic process that gives rise to classic dermal CLH. There is controversy regarding whether Kimura disease and ALHE are variants of the same disorder, although most favor the concept that they are distinct clinicopathologic entities despite some clinicopathologic overlap. The terms epithelioid hemangioma and pseudopyogenic granuloma have been used as synonyms for ALHE. Some regard ALHE essentially as a malformation of blood vessels caused by an underlying arteriovenous shunt. They consider the CLH-like aspects of the lesional infiltrate to be a secondary feature. Those who believe that ALHE should be classified as a separate disorder argue that, compared with the lesions of Kimura disease, ALHE lesions tend to be smaller and more superficial (centered in the dermis rather than the subcutis) and exhibit a more prominent vascular hyperplasia, characterized by small blood vessels lined by plump endothelial cells with abundant cytoplasm and sometimes atypical nuclei . In addition, there is often evidence of arteriovenous anastomoses, the lymphoid infiltrate is less extensive, secondary lymphoid follicles are present in only a minority of cases, and lymphadenopathy is usually absent. Patients with both AHLE and Kimura disease have been shown to harbor dominant clonal T-cell populations in some cases. Clinical Findings Kimura disease presents as solitary or multiple nodules up to 10 cm in diameter centered in the subcutis, most commonly involving the head and neck.Peripheral eosinophilia and regional lymphadenopathy are characteristic. AHLE tends to present with multiple smaller, more superficial intradermal papulonodules that are typically unilateral. Salivary glands, lymph nodes, and other cutaneous sites can also be affected in either disorder, although such locations are more typical of Kimura disease. Histopathologically, the dermis and/or subcutis exhibit hyperplasia of small blood vessels lined by plump endothelial cells similar to those present in the high endothelial venules of lymphoid tissues. These venules are a major point of lymphocyte trafficking between the blood and the paracortical T-cell domain of lymph nodes. Surrounding these hyperplastic vessels is a dense infiltrate composed of small lymphocytes, plasma cells, histiocytes, and eosinophils. The latter are typically prominent but may be absent in some cases. There are usually multiple secondary lymphoid follicles with prominent germinal centers, particularly in the subcutaneous lesions. In general, lesions are more superficial and the vascular features are more prominent in AHLE, whereas lesions are deeper and the lymphoid features are more prominent in Kimura disease.
Differential Diagnosis Kimura disease, which generally forms deeper, larger lesions, needs to be distinguished from CBCL, sinus histiocytosis with massive lymphadenopathy, soft tissue tumors, and subcutaneous deposits of metastatic carcinoma . AHLE, which has smaller, more superficial lesions, should be differentiated from CLH, CBCL, hemangioma, angiosarcoma, pyogenic granuloma, nodular Kaposi sarcoma, bacillary angiomatosis, and bartonellosis. Many of these entities have distinctive histopathologic features. The distinguishing features of CLH and CBCL have been discussed earlier (see Differential Diagnosis under Cutaneous Lymphoid Hyperplasia).
Complications Kimura disease has been associated with lichen amyloidosis and renal disorders such as nephrotic syndrome.
Differential Diagnosis of Kimura Disease and Angiolymphoid Hyperplasia (AHLE)
Most Likely
Consider
Always Rule Out
Prognosis and Clinical Course Some cases, such as those associated with dominant T-cell clonality, have exhibited a chronic clinical course marked by multiple recurrences and resistance to treatment.
Treatment The treatment of Kimura disease and AHLE is not well established because of the rarity of the disorders. Many approaches have been tried in only a limited number of cases.. Topical treatments are used mainly for AHLE. Local radiation therapy has been reported to be superior to surgery and corticosteroids for treatment of Kimura disease |