|
Incontinentia pigmenti =السلس الصباغي |
 |
 |
 |
|
Incontinentia Pigmenti
Incontinentia pigmenti (IP) is an X-linked dominantly inherited disorder. Females with the abnormal gene on only one of their two X chromosomes are heterozygous for this condition and are not severely affected, but males with the abnormal gene on their single X chromosome are hemizygous for this condition and hence are so severely affected that they typically die in utero. This explains the predominance of female patients with this disorder . To date, over 40 male patients with IP have been reported . Male patients may survive either through hypomorphic mutations, as in cases of genetic mosaicism, or through the presence of a compensatory X chromosome, as in cases of 47,XXY or Klinefelter syndrome . The familial form of this disorder, IP2 (or
|
|
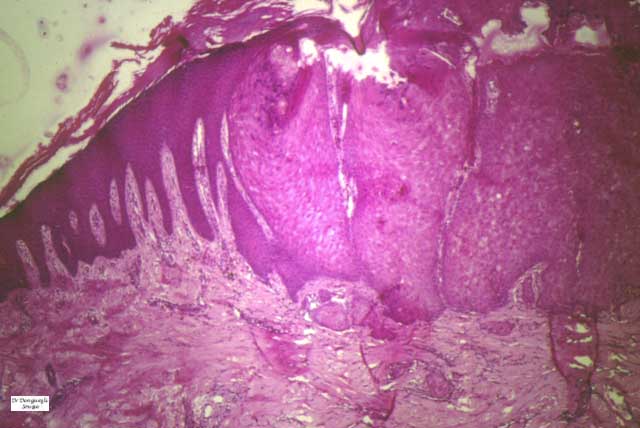
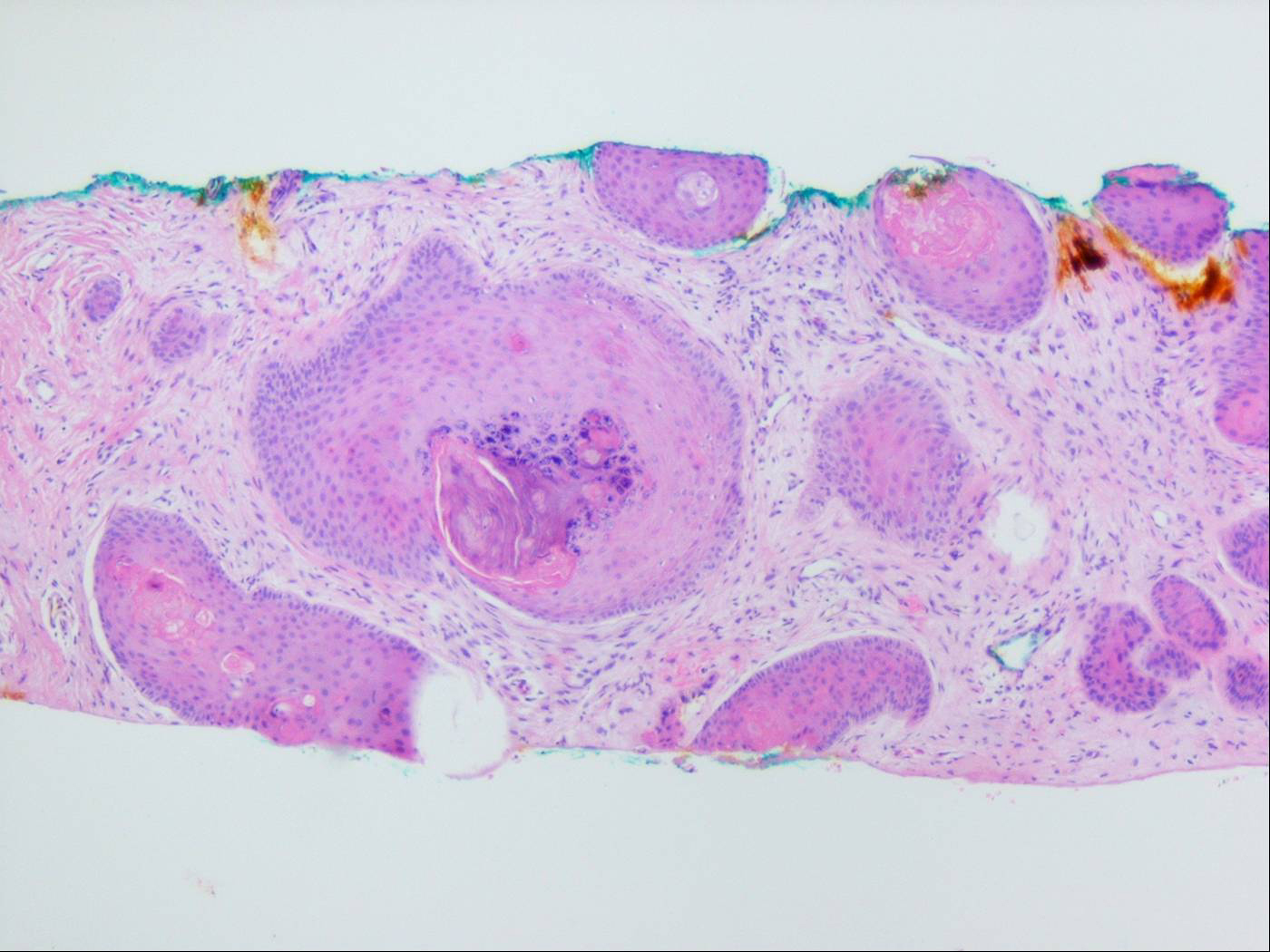
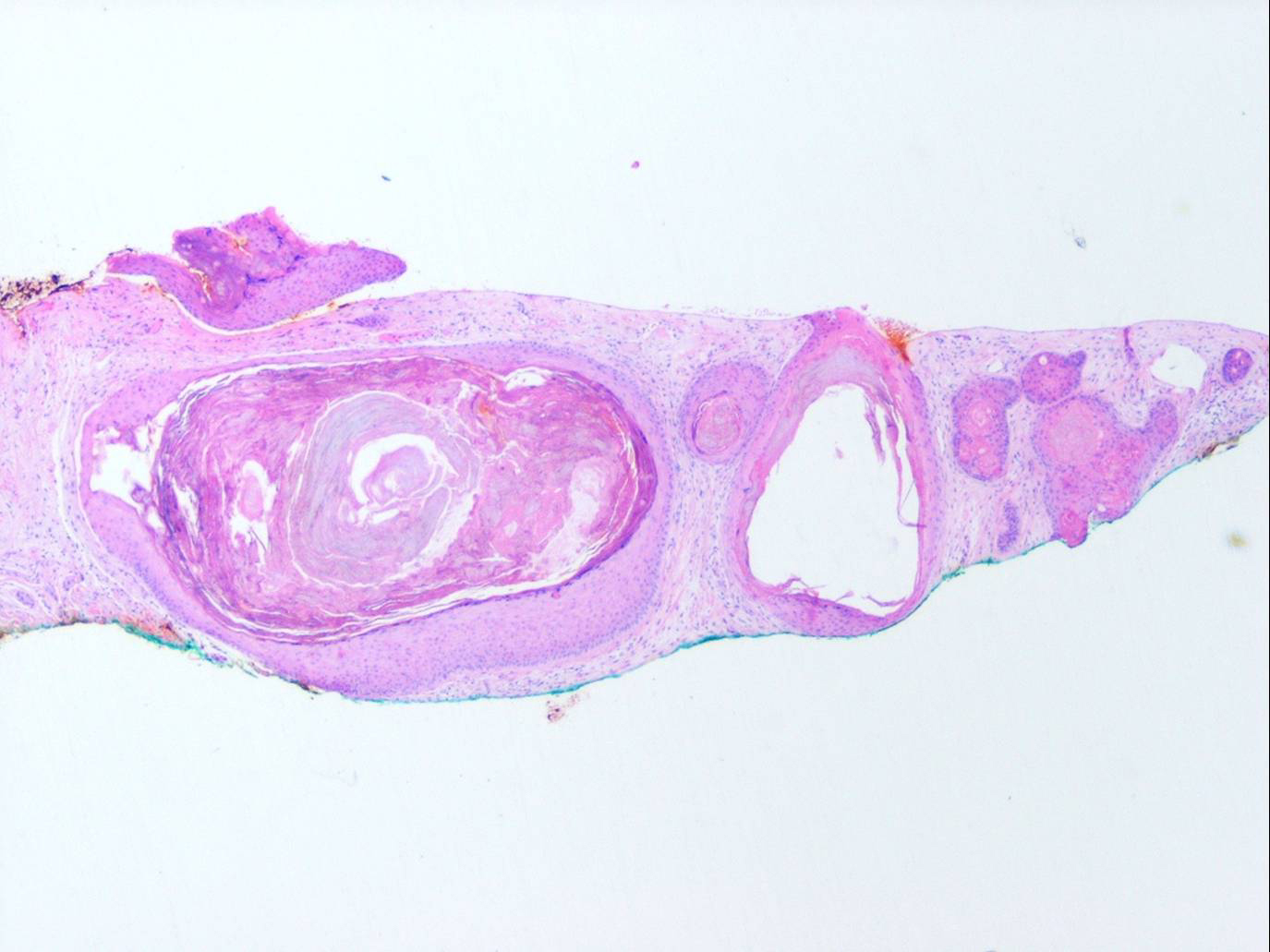
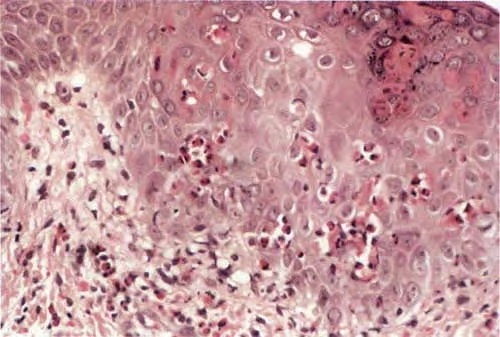
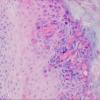
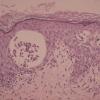
The alterations in the second stage consist of acanthosis, irregular papillomatosis, and hyperkeratosis. Intraepidermal keratinization, consisting of whorls of keratinocytes and of scattered dyskeratotic cells, is often more pronounced than in the first stage. The basal cells show vacuolization and a decrease in their melanin content. The dermis shows a mild, chronic inflammatory infiltrate intermingled with melano-phages. This infiltrate extends into the epidermis in many places.
|
|
classical incontinentia pigmentosa), is localized to the Xq28 region . It is due to a mutation in the IKK-gamma gene as part of the NEMO complex.
|
|
The disorder has four stages. The first stage, consisting of erythema and bullae arranged in lines, either is present at birth or starts shortly thereafter. The extremities are predominantly affected. There is also marked blood eosinophilia. In the second stage, which occurs after about 2 months, the vesicular lesions gradually are superseded by linear, verrucous lesions that persist for several months. As the verrucous lesions subside, widely disseminated areas of irregular, spattered, or whorled pigmentation develop. This pigmentation, representing the third stage, is most pronounced on the trunk (Fig. 6-42A). It diminishes gradually after several years and may even clear completely. The fourth stage is seen in adult females. Subtle, faint, hypochromic or atrophic lesions in a linear pattern are most apparent on the lower extremities.
|
|
In about 80% of the cases, IP is associated with various congenital abnormalities, particularly of the central nervous system, eyes, and teeth. Partial alopecia at the vertex is also often seen .
|
|
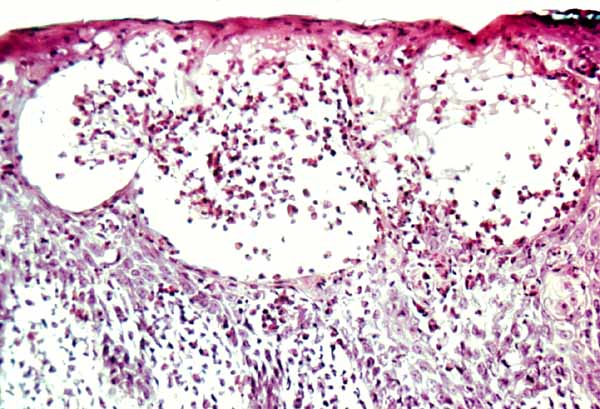
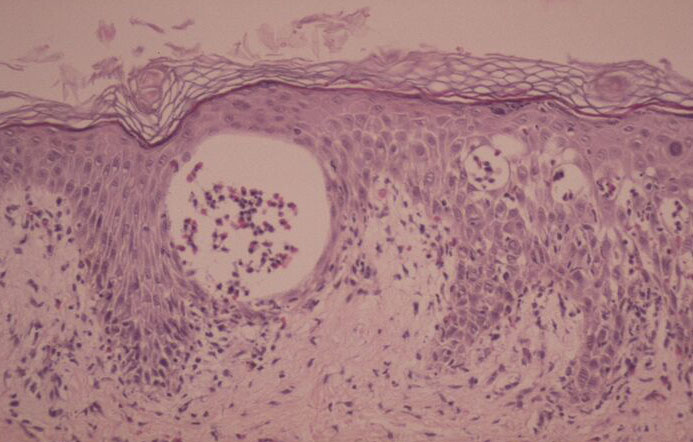
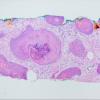
Histopathology.
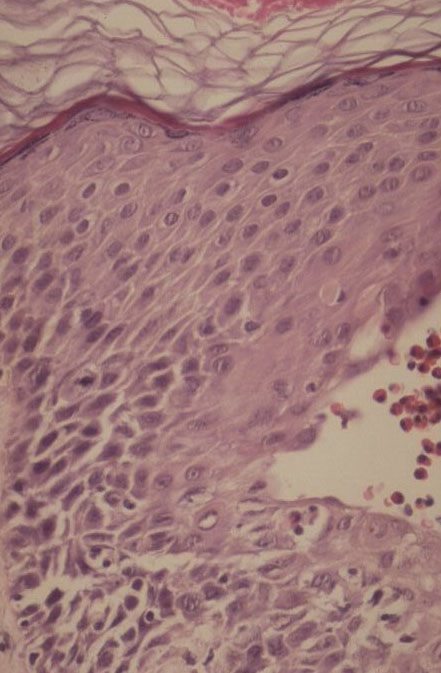
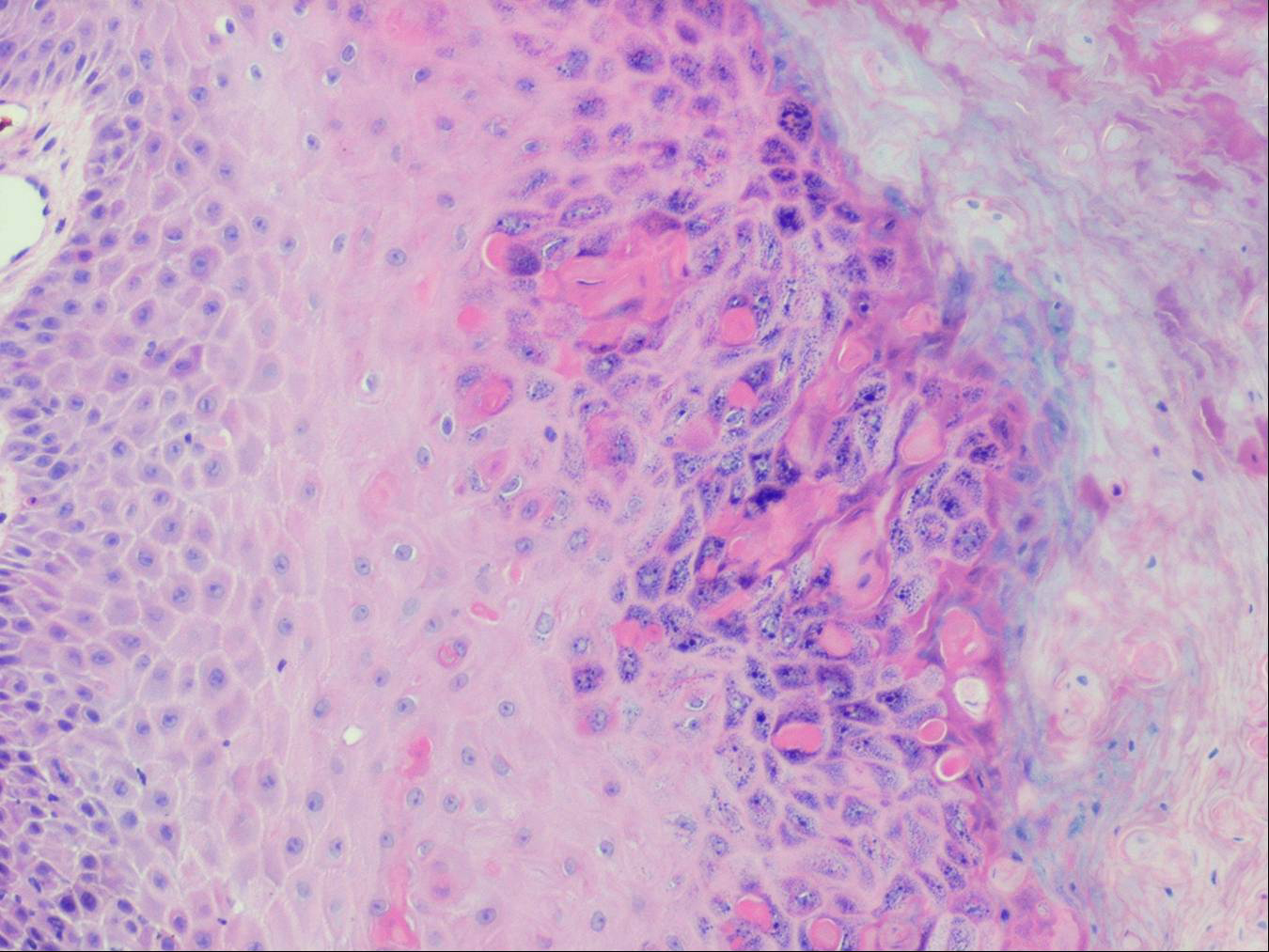
The vesicles seen during the first stage arise within the epidermis and are associated with spongiosis. They are of the type seen in dermatitis . However, they differ from the vesicles of dermatitis by the numerous eosinophils within them and around them in the epidermis (eosinophilic spongiosis) . The epidermis between the vesicles often shows single dyskeratotic cells and whorls of squamous cells with central keratinization. Like the epidermis, the dermis shows an infiltrate containing many eosinophils and some mononuclear cells.
|
|
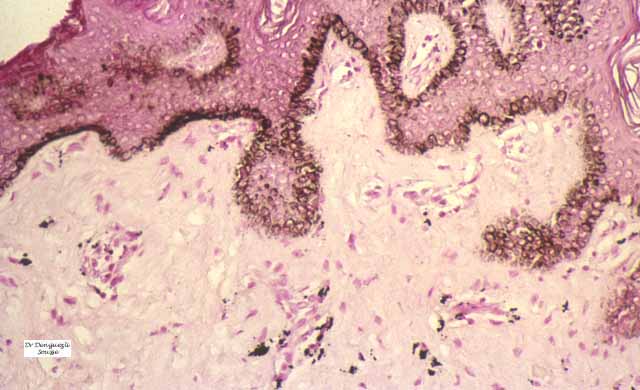
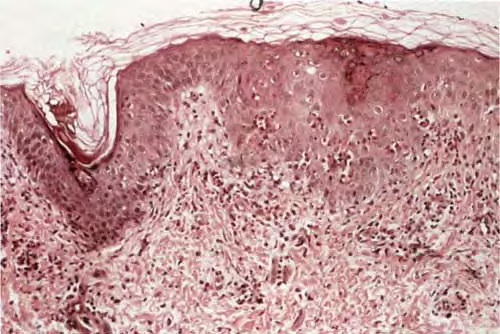
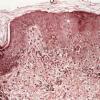
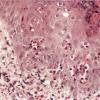
The areas of pigmentation seen in the third stage show extensive deposits of melanin within melanophages located in the upper dermis. Usually, this dermal hyperpigmentation is found in association with a diminution of pigment in the basal layer, the cells of which show vacuolization and degeneration . In some cases, however, the cells of the basal layer contain abundant amounts of melanin .
A different pattern has recently been described on the skin of the legs of an infant in whom the vesiculation had produced superficial scarring and depigmentation. The light-colored skin lacked melanocytes and appendages as the result of scarring, and the darker skin showed a normal degree of pigmentation without incontinence of pigment .
|
|
Pathogenesis
. The fact that the first two stages of IP are seen predominantly on the extremities and the third stage mainly on the trunk has led to the assumption by some authors that
|
|
the pigmentary changes of the third stage occur independently of the bullous and verrucous lesions of the first two stages and represent some sort of nevoid anomaly. However, electron microscopic studies have revealed common features, albeit to varying extents, in all three stages of IP and thus suggest that the three stages are related to
|
|
each other . Even in the first stage, many keratinocytes and melanocytes show degenerative changes resulting in the migration of macrophages to the epidermis, where they phagocytize dyskeratotic keratinocytes and melanosomes. Subsequently, the macrophages return to the dermis (EM 6). The macrophages seen in the dermis in the second and third stages contain many melanosome complexes and thus are easily recognizable as melanophages even by light microscopy, whereas the macrophages in the first stage contain only few melanosome complexes and therefore can be identified as melanophages only in the electron microscope . The phagocytosis of melanin by dermal macrophages in the first stage of the disease and the presence of dyskeratotic keratinocytes in the epidermis during all three stages of the disease have been confirmed.
|
The presence of eosinophils in epidermal and dermal infiltrates can be explained by the presence in the early vesicular stage of basophils, which release eosinophil chemotactic factor of anaphylaxis . Eosinophil chemotactic activity has been demonstrated in patients with IP in the blister fluid and in eluates of crusted scales overlying the lesions
|