|
Erythema Multiforme Stevens Johnson Syndrom
There has been controversy in the literature regarding the clinical definitions of EM, SJS, and TEN and whether they are distinct entities or represent a spectrum of one disease process. While EM major and SJS were once considered synonymous, many now consider EM and SJS to be separate diseases . SJS and TEN are widely but not universally regarded as a continuum.
|
|
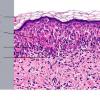
EM, as classically described by von Hebra, is a benign, self-limited condition with symmetric, fixed lesions, some of which evolve into typical targets composed of three concentric rings. The lesions are located primarily on the extremities (Fig. 9-26A). Bullous EM is a more severe form, which was defined by an international consensus group in 1993 as having typical targets or raised atypical targets with <10% of body surface area detachment .
|
|
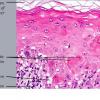
Patients with SJS often present with fever and malaise and develop a cutaneous eruption consisting of "flat atypical targets," or erythematous or purpuric macules, many with central epidermal necrosis or blister formation. The lesions usually start on the trunk and spread centrifugally. Again, epidermal detachment is <10% of the body surface area .
|
|
TEN, also referred to as Lyell's syndrome, is characterized by widespread, full-thickness epidermal necrosis involving >30% of the body surface area . These patients also have systemic symptoms and may initially present with diffuse erythema and skin tenderness, followed by the development of large, flaccid bullae and detachment of the epidermis in sheets . SJSfTEN overlap is used to refer to patients with epidermal detachment between 10% and 30% of the body surface area . TEN has a high mortality rate because offluid loss and sepsis.
|
|
Mucosal involvement (oral, ocular, and/or genital) is common in all of these severe acute bullous diseases and is a serious cause of morbidity. Mycoplasma pneumoniae infection has been associated with severe mucositis without skin lesions, which has been referred to by some as atypical SJS , while others argue that the classification of SJS requires cutaneous involvement .
EM, which may be recurrent, is most commonly associated with herpes simplex infection . Other infections, (Epstein-Barr virus , cytomegalovirus , and Lyme disease ), and rarely drugs, have been implicated in EM. SJS is most commonly drug-induced , except in
|
|
children where the majority of cases have been associated with infection, notably M. pneumoniae ). Immunizations are another etiology to consider. TEN is almost always attributed to drugs, and only rare cases have been thought to have an infectious etiology . The most commonly implicated drugs include NSAIDs, sulfonamides and other antibiotics, anticonvulsants, antiretrovirals, and allopurinol .
|
|
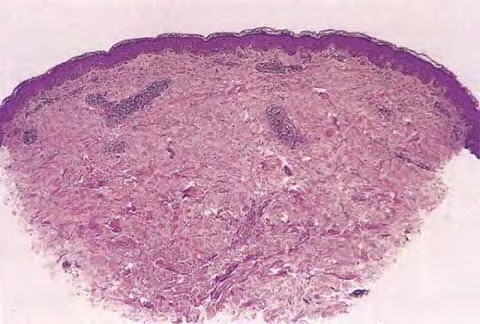
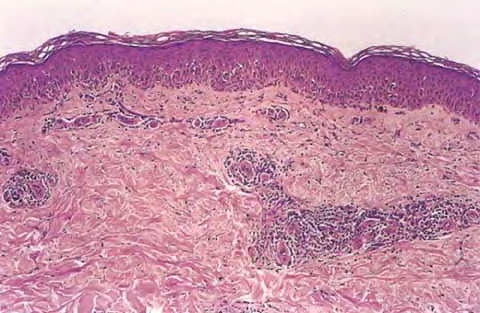
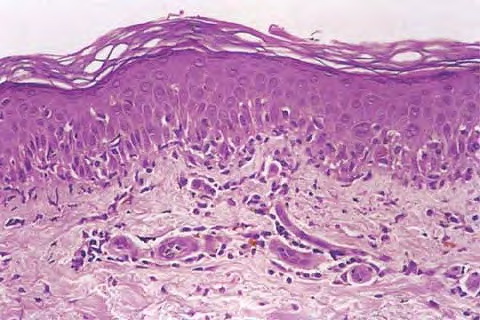
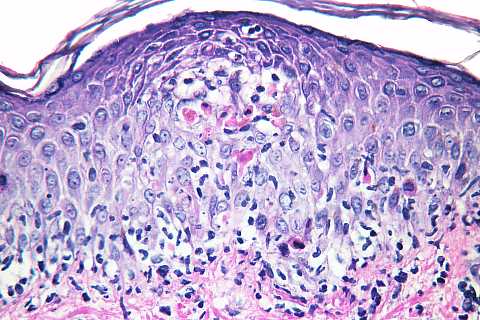
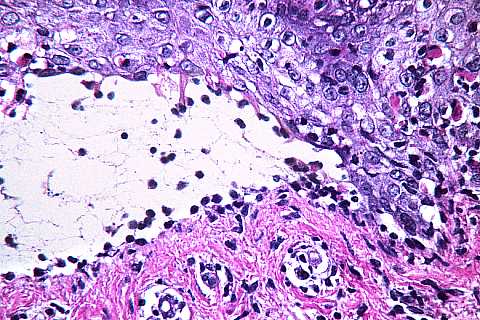
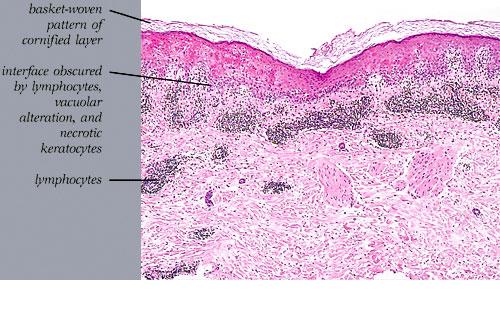
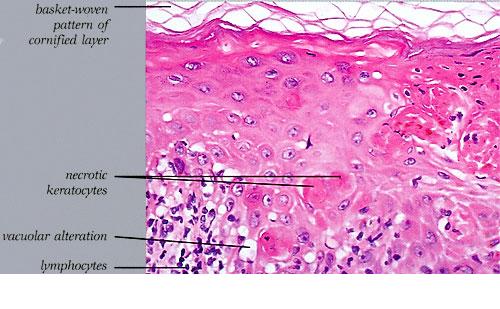
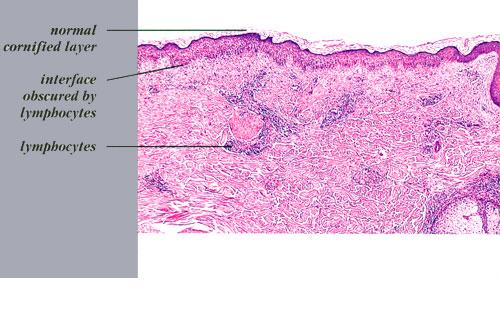
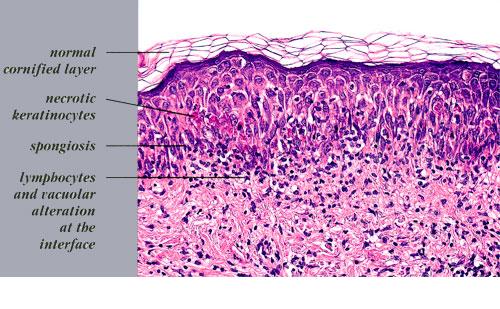
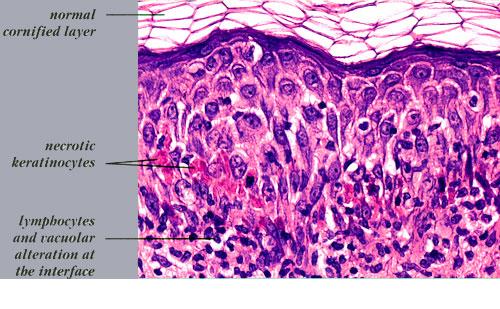
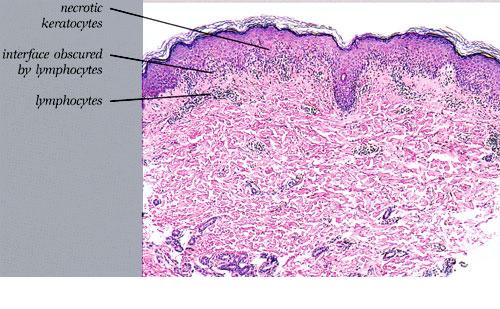
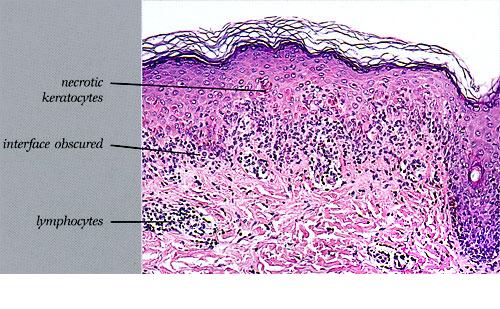
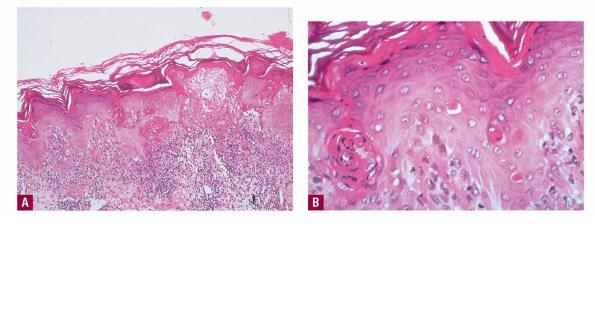
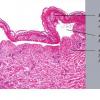
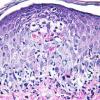
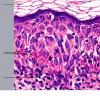
Histopathology. EM is considered the prototype of the vacuolar form of interface dermatitis . The early changes include vacuolization of the basal cell layer; tagging of lymphocytes along the dermal-epidermal junction; and a sparse, superficial, perivascular lymphoid infiltrate . Necrosis of individual keratinocytes in the basal unit occurs, which is the hallmark of EM. Because of its acute nature, there is an orthokeratotic stratum corneum. Mild spongiosis, papillary dermal edema, and extravasation of red blood cells are seen. As the lesion becomes more developed, there is a moderate lichenoid infiltrate of Iymphohistiocytes at the dermal-epidermal junction with exocytosis. More apoptotic keratinocytes within and above the basal epidermal layer are present. The
|
|
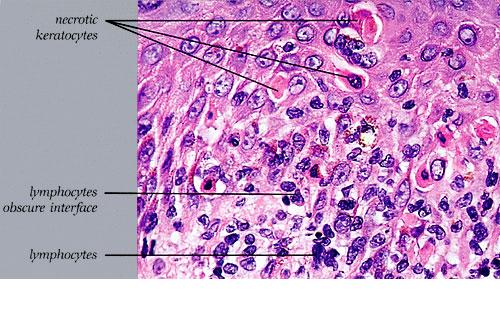
intensity of epidermal necrosis varies from vacuolated individual keratinocytes surrounded by lymphocytes (satellite cell necrosis) at the basal unit to confluent necrosis in association with intraepidermal and subepidermal vesicles. The dermal infiltrate comprises lymphocytes and histiocytes. Eosinophils may also be present. Although one study has noted a significant number of eosinophils in drug-induced EM, this has not been noted by others. In the authors' estimation, a generous number of eosinophils exclude EM. One study has found that an acrosyringium concentration of apoptotic keratinocytes in EM is a clue to a drug etiology .
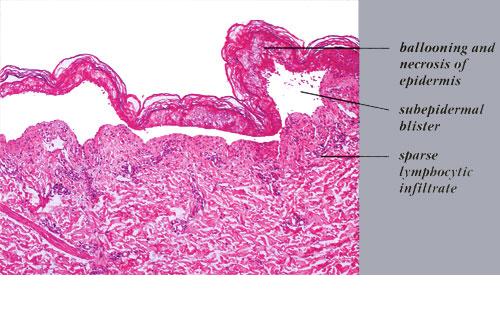
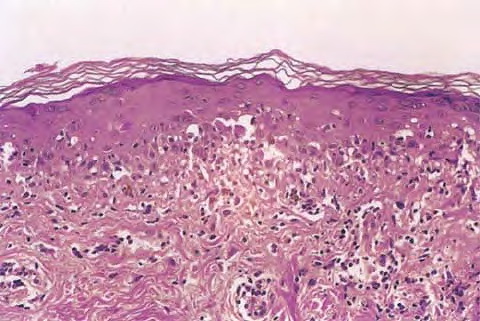
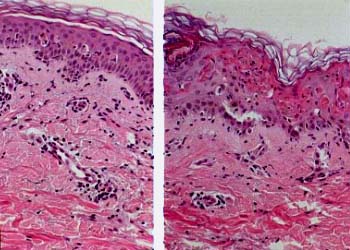
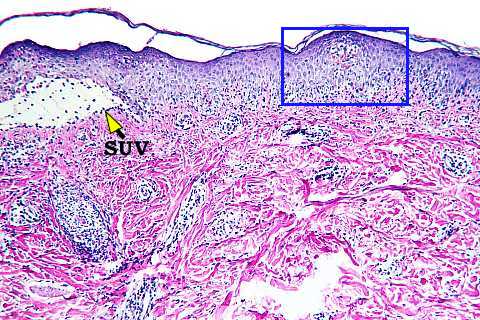
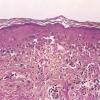
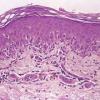
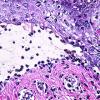
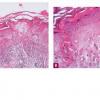
In early lesions of SJSITEN, apoptotic keratinocytes are observed scattered in the basal layer of the epidermis. In established lesions, there are numerous necrotic keratinocytes, even full-thickness epidermal necrosis, and a subepidermal bulla. The dermal inflammatory infiltrate is sparser in TEN than in EM (Fig. 9-278). Extravasated erythrocytes are commonly found within the blister cavity. Melanophages within the papillary dermis occur in late lesions. Eccrine epithelium shows a variety of changes from basal cell apoptosis to necrosis of the duct.
|
|
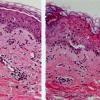
In general, EM shows less epidermal necrosis, more dermal inflammation, and exocytosis, whereas SJS and TEN reveal more epidermal necrosis, less dermal inflammation, and exocytosis. However, due to the overlapping histologic features among EM, SJS, and TEN, histologic examination-while important for recognizing the spectrum of disorders-is not reliable for classifying the disease. Correlation with clinical presentation is essential.
|
|
IF Testing. In many patients with EM, deposits of IgM and C3 are found in the walls of the superficial dermal vessels. Granular deposits of C3, IgM, and fibrinogen may also be present along the dermal-epidermal junction. Nonspecific deposition of immune reactants in apoptotic or necrotic keratinocytes may be observed in other disorders with apoptosis, lymphocyte satellite necrosis, and epidermal necrosis.
|
|
Pathogenesis. EM appears to result from a cell-mediated immune reaction. In the case of herpes simplex, polymerase chain reaction and in situ hybridization have detected herpes simplex virus (HSV) DNA within lesions of EM . The virus remains in the skin for up to 3 months after the lesions have healed . Some authors hypothesize that disease development begins with deposition and expression of HSV genes, leading to recruitment of HSV-specific CD4+ T cells with production of INF-y. This step initiates an inflammatory cascade that includes increased infiltration of leukocytes, monocytes, NK cells, and T cells . The infiltrate consists largely of CD4+ (helper) lymphocytes in the dermis and CD8+ (cytotoxic) cells in the epidermis. The mononuclear cells that are associated with necrotic keratinocytes in the process referred to as satellite cell necrosis are largely CD8+ cytotoxic lymphocytes similar to those occurring in GVHD. The pathogenesis of TEN remains unclear but is thought to be
mediated by cytotoxic T lymphocytes. As is EM, mainly CD8+ cells are found in the epidermis and blister fluid, while CD4 + cells are in the dermis. Macrophages are also thought to play an important role, along with cytokines such as tumor necrosis factor-a (TNF-a). In vitro studies suggests Fas-FasL and other death receptors, as well as perforin/granzyme trigger apoptosis in TEN .
|
|
Ultrastructural Study. The basal lamina is located on the floor or the roof of the blister. The basal cells show marked intracytoplasmic damage with a loss of organelles. Neutrophils and macrophages, which are rich in Iysosomes, are present in the lower epidermis phagocytizing the damaged keratinocytes. In the mid-epidermis, large, electron-dense, dyskeratotic bodies correspond to the cells with eosinophilic necrosis seen by light microscopy. The damaged epidermal cells often contain few or no organelles. Large granular lymphocytes have been identified within the epidermis in close contact with keratinocytes, a finding that supports cell-mediated
|
|
cytotoxic injury to keratinocytes .
|
|
Differential Diagnosis.
Necrotic keratinocytes are also a characteristic feature in drug eruption, especially fixed drug eruptions, pityriasis lichenoides, connective tissue disease, subacute radiation dermatitis, phototoxic dermatitis, acute GVHD, and viral exanthems. Clinicopathologic correlation will help in their distinction. In patients with widespread desquamation or detachment, the clinical differential diagnosis includes TEN and SSSS. Whereas the former involves subepidermal separation, the latter results from separation of the epidermis subcorneally or within the granular layer. Frozen section evaluation of the blister roof is a rapid diagnostic tool to determine the level of the split.
|
|