|
Eosinophilic pustula folliculitis = التهاب الاجربة الشعرية البثري بالحمضات |
 |
 |
 |
|
Eosinophilic Pustular Folliculitis
Ofuji originally described eosinophilic pustular folliculitis (EPF) in immunocompetent Japanese patients as itchy follicular papules and pustules arranged in arcuate plaques with central healing and peripheral spread . Although most reported cases have been from Japan, the condition is now known to be geographically more widespread. Lesions typically involve seborrheic areas, including the face, trunk, and upper arms, with documented reports of extrafollicular lesions of the palms and soles . Moderate leukocytosis and eosinophilia in the peripheral blood may be present. There is usually spontaneous healing over months to years . There are reports of the eruption in children ), including neonates , and in this subset lesions occur predominantly on the scalp. Scarring alopecia of the scalp in an adult has been reported . Although a cause has not been identified, rare medication-induced cases have been described due to carbamazepine and allopurinol , after patch testing with minocycline and indeloxazine hydrochloride , and after prolonged treatment with oral corticosteroids in a patient with pustulosis palmoplantaris . Cases have been associated with nevoid basal cell carcinoma syndrome , hepatitis C infection , and infestations
|
|
Lesions with similar histology are well documented in patients with HIV infection , including children with HIV , and other immunocompromised conditions, such as myelodysplastic syndrome , non-Hodgkin's lymphoma , B-cell chronic lymphatic leukemia , polycythemia vera , after bone marrow transplantation , and after autologous peripheral blood stem-cell transplantation . There appear to be enough clinical dissimilarities from the disorder described by Ofuji to consider HIV-associated disease a distinct entity, and use of the terms eosinophilic folliculitis or HIV-associated eosinophilic folliculitis was recommended to reflect this . Another classification scheme proposed the designations classical, infancy associated, and immunosuppression associated (mostly HIV) . In HIV patients, lesions tend to be urticarial papules with less tendency to become pustular, and leukocytosis is less common . They are most commonly found on the face, scalp, and upper trunk and often are excoriated.
|
|
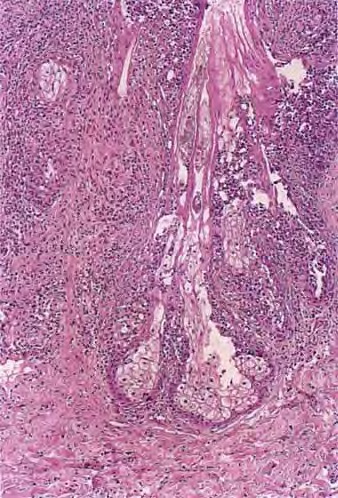
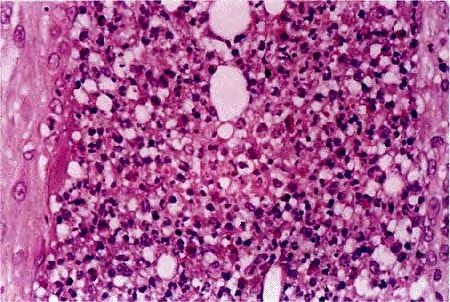
Histopathology.
In Ofuji's disease, there is exocytosis of eosinophils into a spongiotic follicular infundibulum and accompanying sebaceous gland, eventually forming eosinophilic micropustules . The epidermis adjacent to the affected follicle may contain lymphocytes and eosinophils, with the latter aggregating into small eosinophilic pustules that are subcorneal or intraepidermal; these epidermal changes reflect the histologic picture seen in palmoplantar lesions, where follicles are absent . In more inflamed lesions neutrophils may be present . In the dermis, there are perivascular and interstitial infiltrates of lymphocytes and numerous eosinophils, which may surround sweat glands. Associated follicular mucinosis has been reported .
|
|
A study of 52 biopsies in 50 HIV-positive patients best described the histology of HIV-associated eosinophilic folliculitis . Perifollicular and intrafollicular lymphocytes and eosinophils are concentrated about the isthmus, and may involve the sebaceous duct. There is spongiosis of the follicular epithelium. Eosinophils and lymphocytes may be seen aggregating in the hair canal, but neutrophils are rare. In early lesions, lymphocytes may predominate and be distributed perifollicularly and interstitially. In more developed lesions, dermal inflammation diminishes and perifollicular/follicular inflammation increases. Less common findings include inflammation of the sebaceous gland, eosinophilic pustules, and follicular rupture (128). Dense eosinophilic infiltrates with degranulation and flame figures, resembling Well's syndrome, may sometimes be seen. A small number of macrophages can be present. Bacteria, yeast, or Demodex may be identified, albeit away from the areas of inflammation. Because the disorder is highly pruritic, excoriation is a common secondary finding.
|
|
Features that may help to distinguish suppurative folliculitis in HIV-positive patients from HIV-associated eosinophilic folliculitis have been described; suppurative folliculitis in HIV-positive patients more commonly shows an infiltrate dominated by neutrophils and macrophages, the presence of microorganisms amid the inflammation, and rupture of the involved follicle. The use of transverse histologic sections has been advocated over vertical sections for increasing diagnostic sensitivity and demonstrating the key pathologic findings in HIV-associated eosinophilic folliculitis .
|
|
In another study of three patients with EPF, serum levels of interferon-y and IL-2, -4, and -6 were measured before and after successful treatment with indomethacin . Investigators found elevated IL-4 in the EPF patients, which remained unchanged after treatment, and increased interferon-y with disease remission. Decreased expression of IL-5 mRNA in peripheral blood mononuclear cells was demonstrated after the disease was controlled in two EPF patients undergoing treatment with interferon-y ; IL-5 is responsible for the growth and differentiation of eosinophils.
|
|
Ultrastructurally, in EPF lesions characterized by an infundibular pustule, acantholytic outer root sheath keratinocytes showed desmosomal cleavage with microvilli formation, and some contained sebaceous lipid droplets . Apposition of T lymphocytes and Langerhans cells was seen.
|
|
Pathogenesis. The cause of Ofuji's disease (EPF) is not known. Although the prevalence in Japan could not be explained by HLA patterns , the occurrence in brothers in the neonatal period hints at some inherited predisposition or possibly an infectious etiology .
The perivascular infiltrating cells in EPF were found to be mostly T lymphocytes, with some CD68+ myelomonocytic cells, and most of the eosinophils were positive for eosinophil cationic protein . A moderate increase in the number of tryptase-positive, chymase-negative mast cells, the type predominantly found in lung and small intestine, was noted around hair follicles and sebaceous glands . A study of Ofuji's disease found markers of sebaceous differentiation to be decreased or absent, whereas follicular differentiation markers were expressed normally .
|
|
In the differential diagnosis, eosinophilic follicular pustules may be seen in erythema toxicum neonatorum, and intraepidermal eosinophilic vesicles can be seen both in acropustulosis and the vesicular phase of incontinentia pigmenti. However, the clinical presentation of these conditions would generally be significantly different than that in EPF, although it has been suggested that EPF in infants and infantile acropustulosis may be variants of the same disorder . Identical eosinophilic pustular eruptions have been described in association with
|
|
Pseudomonas infection and in fungal infections due to dermatophytes .
|
|
|
|
|