|
Dariers Disease
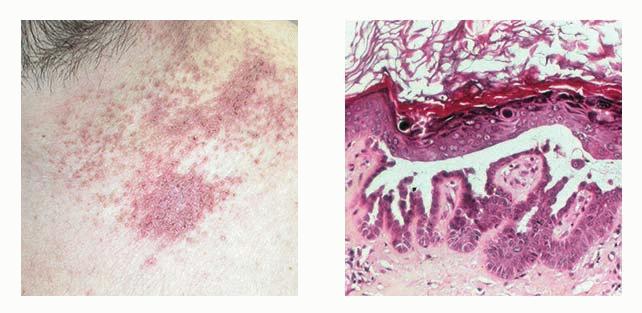
Darier's disease is usually transmitted in an autosomal dominant pattern. It has been found to be due to mutations in the ATP2A2 gene on chromosome T2, which encodes the sarcoplasmic/endoplasmic reticulum calcium pumping ATPase SERCA2 (206). The gene is 12q23-24.1. In typical cases, there is a more or less extensive, persistent, slowly progressive eruption consisting of hyperkeratotic or crusted papules often showing a follicular distribution. By coalescence verrucous, crusted areas may form. The so-called seborrheic areas are the sites of predilection.
|
|
The oral mucosa is involved occasionally . In some cases of Darier's disease, keratotic papules that resemble those seen in acrokeratosis verruciformis of Hopf are found on the dorsa of the hands and feet .
|
|
Special clinical variants of keratosis follicularis are a hypertrophic type, a vesiculobullous type, and a linear or zosteriform type. In the hypertrophic type, widespread, markedly thickened, and hyperkeratotic lesions are seen, especially in the intertriginous areas . In the vesiculobullous type, vesicles and small bullae are seen in addition to papules . In the linear or zosteriform type, usually limited to one side, there are either localized or widespread lesions that may be present at birth but in most cases have arisen in infancy, childhood, or adult life . The question has been raised as to whether this type of lesion represents a linear epidermal nevus with acantholytic dyskeratosis rather than Darier's disease , and the designation acantholytic dyskeratotic epidermal nevus has been suggested . It is quite likely that some of the cases with scattered papular lesions of limited extent arising in adult life and diagnosed as acute, eruptive Darier's disease or acute adult-onset Darier-like dermatosis in reality represented transient acantholytic dermatosis. A recent review on the clinical aspects of this condition has been written .
Histopathology.
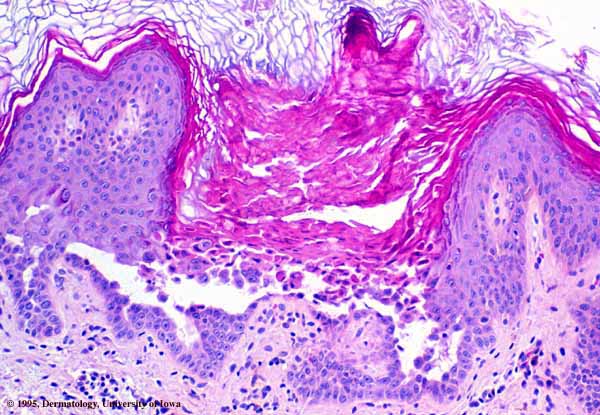
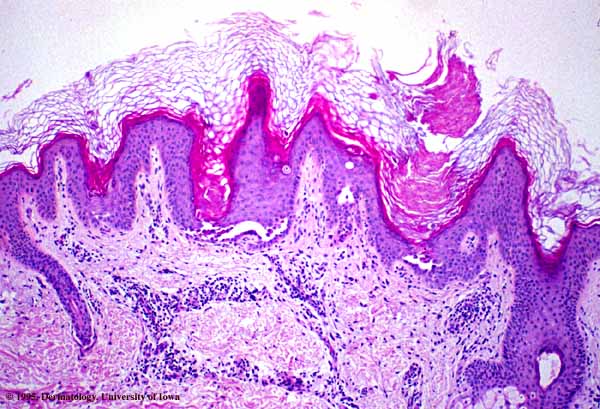
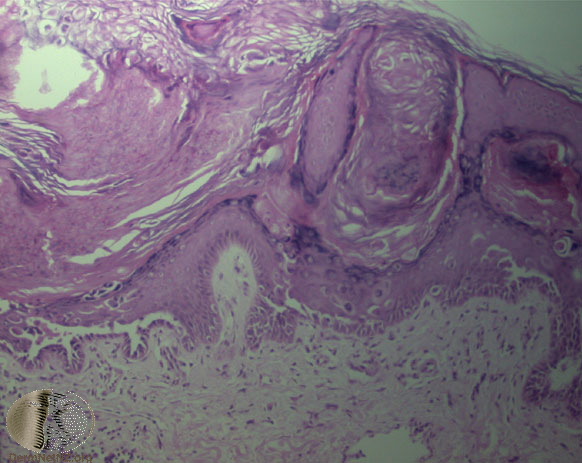
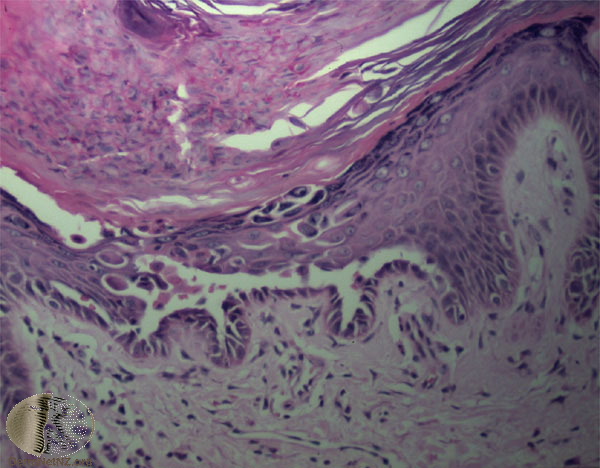
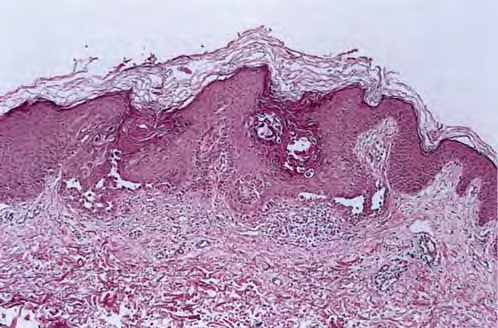
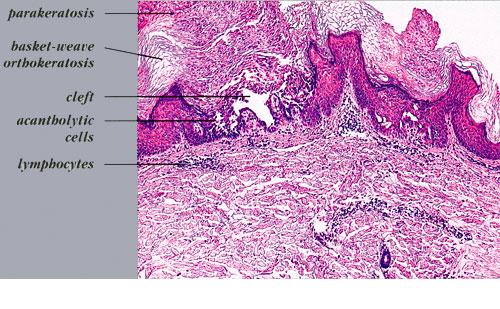
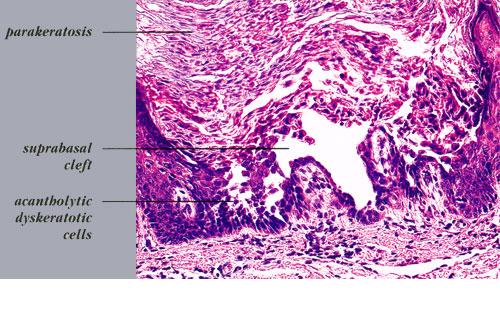
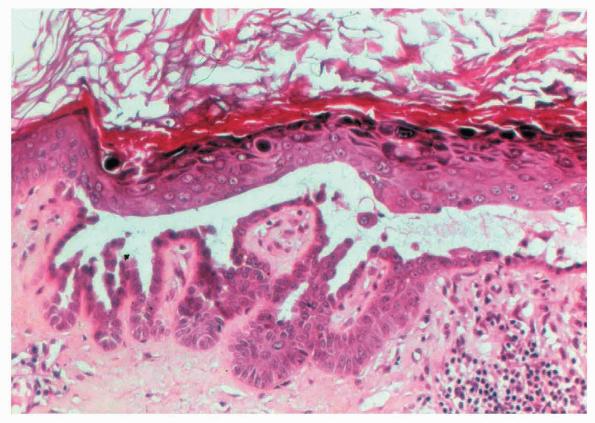
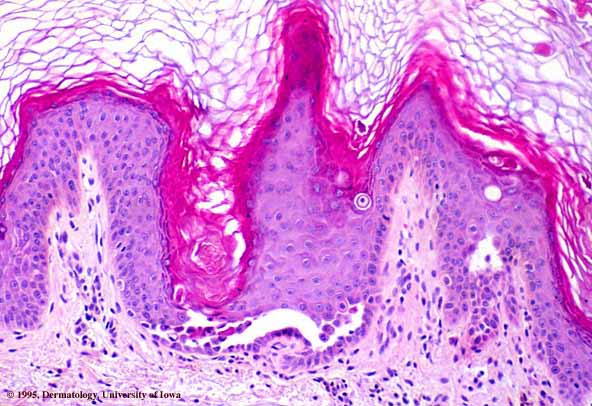
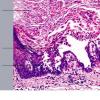
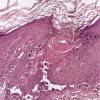
The characteristic changes in Darier's disease include the following: (a) a peculiar form of dyskeratosis resulting in the formation of corps ronds and grains; (b) suprabasal acantholysis leading to the formation of suprabasal clefts or lacunae; and (c) irregular upward proliferation into the lacunae of papillae lined with a single layer of basal cells, so-called villi (Fig. 6-27). There are also papillomatosis, acanthosis, and hyperkeratosis. The dermis shows a chronic inflammatory infiltrate. In some cases, there is downward proliferation of epidermal cells into the dermis.
|
|
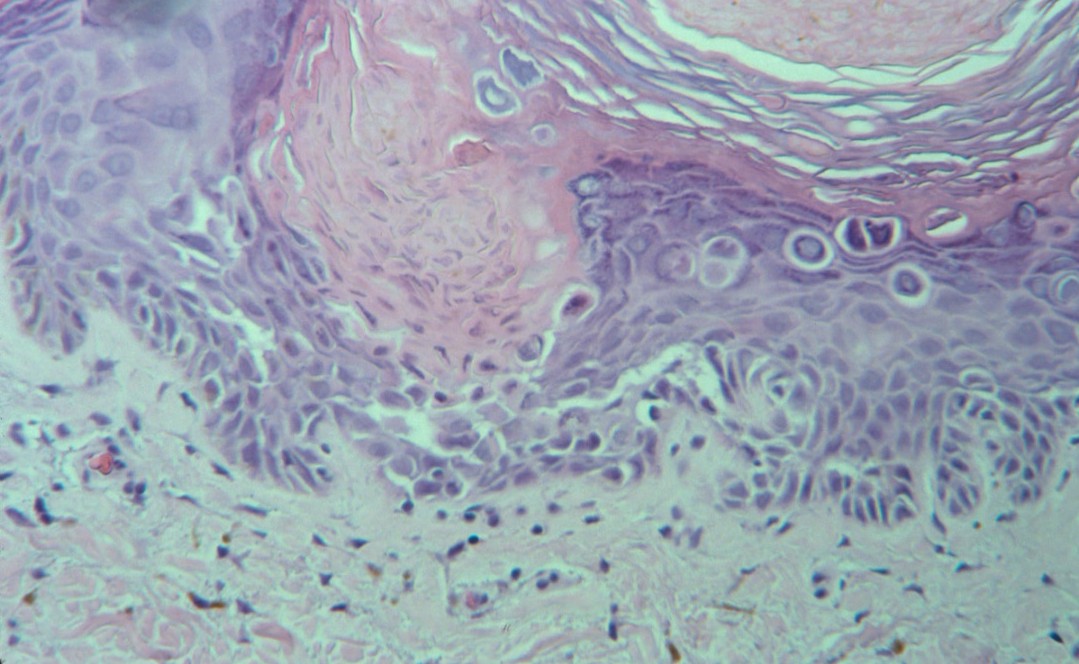
The corps ronds occur in the upper stratum malpighii, particularly in the granular and horny layers; grains are found in the horny layer and as acantholytic cells within the lacunae. Corps ronds possess a central homogeneous, basophilic,
|
|
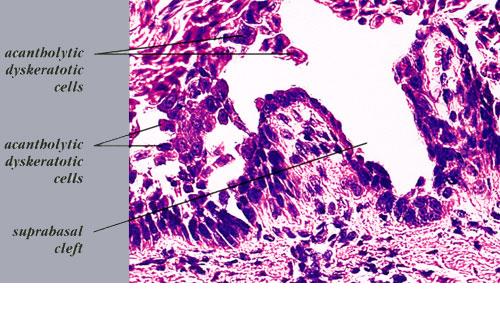
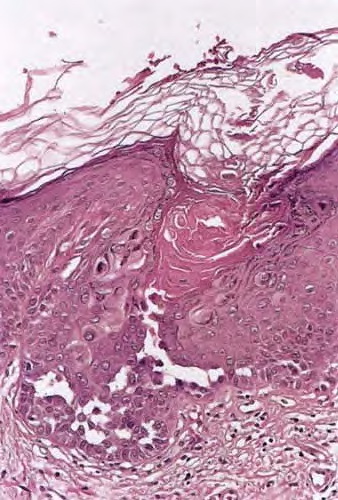
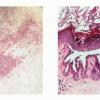
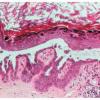
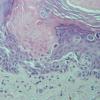
pyknotic nucleus that is surrounded by a clear halo. By virtue of size and the conspicuous halo, corps ronds stand out clearly . Peripheral to the halo lies basophilic dyskeratotic material as a shell . The nonstaining halo in some instances is partially replaced by homogeneous, eosinophilic dyskeratotic material . Compared with the corps ronds, the grains are much less conspicuous. They resemble parakeratotic cells but are somewhat larger. The nuclei of grains are elongated and often grain shaped and are surrounded by homogeneous dyskeratotic material that usually stains basophilic but may stain eosinophilic. The lacunae represent small, slitlike intraepidermal vesicles most commonly located directly above the basal layer. They contain acantholytic cells and show premature partial keratinization. Because of shrinkage, some of them are elongated, and these then appear identical with the grains in the horny layer. The villi projecting into the lacunae may be quite tortuous, so on histologic examination, some of them appear in cross section as rounded dermal structures lined by a solitary row of basal cells .
|
|
Hyperkeratosis and papillomatosis may cause the formation of keratotic plugs, which often fill the pilosebaceous follicles but are found also outside of follicles. That Darier's disease is not exclusively a follicular disorder is also proved by the fact
|
|
that areas devoid of follicles, such as palms, soles, and the oral mucosa, may be affected.
|
|
In hypertrophic lesions of Darier's disease, considerable acanthosis may occasionally be observed, either as proliferations of basal cells or as pseudocarcinomatous hyperplasia. Proliferations of basal cells consist of long, narrow cords composed of two rows of basal cells separated by a narrow lacunar space
|
|
The vesiculobullous lesions, which occur in rare instances, differ from lacunae merely in size; they contain numerous shrunken cells with the appearance of grains .
The keratotic papules that may occur on the dorsa of the hands and feet and that clinically resemble those seen in acrokeratosis verruciform is of Hopf in most instances, on serial sectioning, show mild dyskeratotic changes and often supra basal clefts as well . They are a manifestation of Darier's disease and not of acrokeratosis verruciformis.
|
|
The lesions on the oral mucosa are analogous in appearance to those observed on the skin and thus show lacunae and dyskeratosis, although definite well-formed corps ronds generally are absent .
|
|
The occasional reports of patients having both Darier's disease and familial benign pemphigus or a transition from one of these two diseases to the other are discussed in the differential diagnosis of familial benign pemphigus.
|
|
Pathogenesis. Whereas histologically a distinction between Darier's disease and familial benign pemphigus is generally possible, with dyskeratosis being the predominating factor in Darier's disease and acantholysis in familial benign pemphigus, this distinction is not as clearly evident in electron microscopic examination. The reason for this is that for electron microscopy, only a small specimen can be processed, which in either of the two diseases shows predominantly acantholysis in some instances and dyskeratosis in others and only rarely shows both. In both diseases, however, acantholysis precedes dyskeratosis.
Acantholysis has been thought by some authors to be due to the loss of the intercellular contact layer within desmosomes, both in Darier's disease and in familial benign pemphigus . The two halves of the desmosomes then pull apart, after which the tonofilaments become detached from them. Another group of authors believes that there is some basic defect in the tonofilament-desmosome complex in Darier's disease and in familial benign pemphigus -resulting in separating of tonofilaments from the attachment plaques of desmosomes and subsequently leading to the disappearance of desmosomes and thus to acantholysis. It is likely that both processes take place simultaneously in both Darier's disease and familial benign pemphigus
|
|
The cause for the acantholysis in Darier's disease and familial benign pemphigus is not yet definitely known. Faulty synthesis of the intercellular substance has long been suspected. It seems likely that mutations underlying Darier's disease and Hailey-Hailey disease would affect structural components but both disorders mapped to chromosome regions devoid of any known candidate gene. Furthur studies have suggested that intercellular communication is crucial for epidermal differentiation. This was corroborated when mutations found in ATP2A2 caused Darier's disease and disclosed a role for the SERCA2 pump in the calcium signaling pathway that regulates cell to cell adhesion and differentiation of the epidermis
|
|
In association with the loss of desmosomes, excessive amounts of tonofilaments form within the keratinocytes around the nucleus as thick, electron-dense bundles. A defect of the tonofilaments would best explain the dyskeratotic features of both Darier's disease and familial benign pemphigus. In Darier's disease, in which the dyskeratosis is much more pronounced than in familial benign pemphigus, thick bundles of tonofilaments, often in
|
|
association with large keratohyaline granules, form large aggregates of homogenized dyskeratotic material. The corps ronds, on electron microscopic examination, are characterized by extensive cytoplasmic vacuolization . They show in their center an irregularly shaped nucleus surrounded by a halo of autolyzed electron-lucid cytoplasm and at their periphery a shell of tonofilaments (EM 16) . On electron microscopic examination, the grains are seen to consist of nuclear remnants surrounded by dyskeratotic bundles of tonofilaments.
|
|
In familial benign pemphigus, too, after loss of the desmosomes, excessive amounts of tonofilaments form within the keratinocytes and aggregate around the nucleus as thick, electron-dense bundles, often in a whorling configuration; however, even though dyskeratosis is present, it is less pronounced than in Darier's disease, and most of the keratinocytes keratinize normally, with only very few becoming grains or corps ronds as the result of dyskeratotic degeneration.
|
|
On intralesional injection of tritiated thymidine, one group observed labeling of many acantholytic keratinocytes in familial benign pemphigus but not in Darier's disease, suggesting that in familial benign pemphigus, the epidermal cells participated in the renewal of the epidermis but
|
|
did not do so in Darier's disease, probably because these cells were undergoing keratinization. However, another group could not confirm this observation.
|
|
Differential Diagnosis
. Although acantholytic dyskeratosis in association with corps ronds is highly characteristic of Darier's disease, it occurs also in several other conditions : in warty dyskeratoma, a solitary lesion with a deep central invagination; in transient or persistent acantholytic dermatosis, in which the lesions consist of discrete papules; in focal acantholytic dyskeratoma, manifesting itself as a solitary papule; and as an incidental small focus in a variety of unrelated lesions. Occasionally, a few corps ronds are seen also in familial benign pemphigus .
|
|