
Colloid Milium
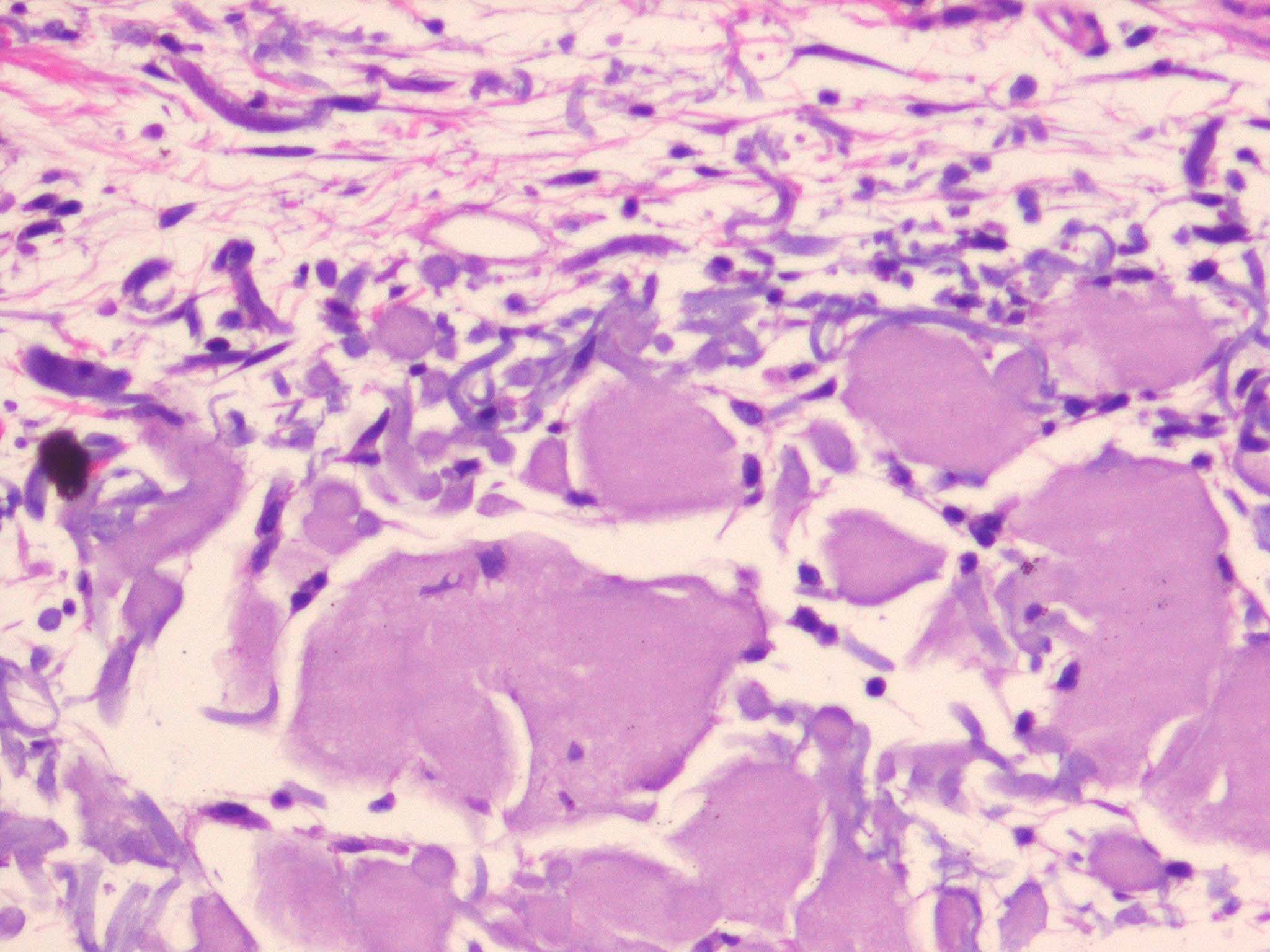
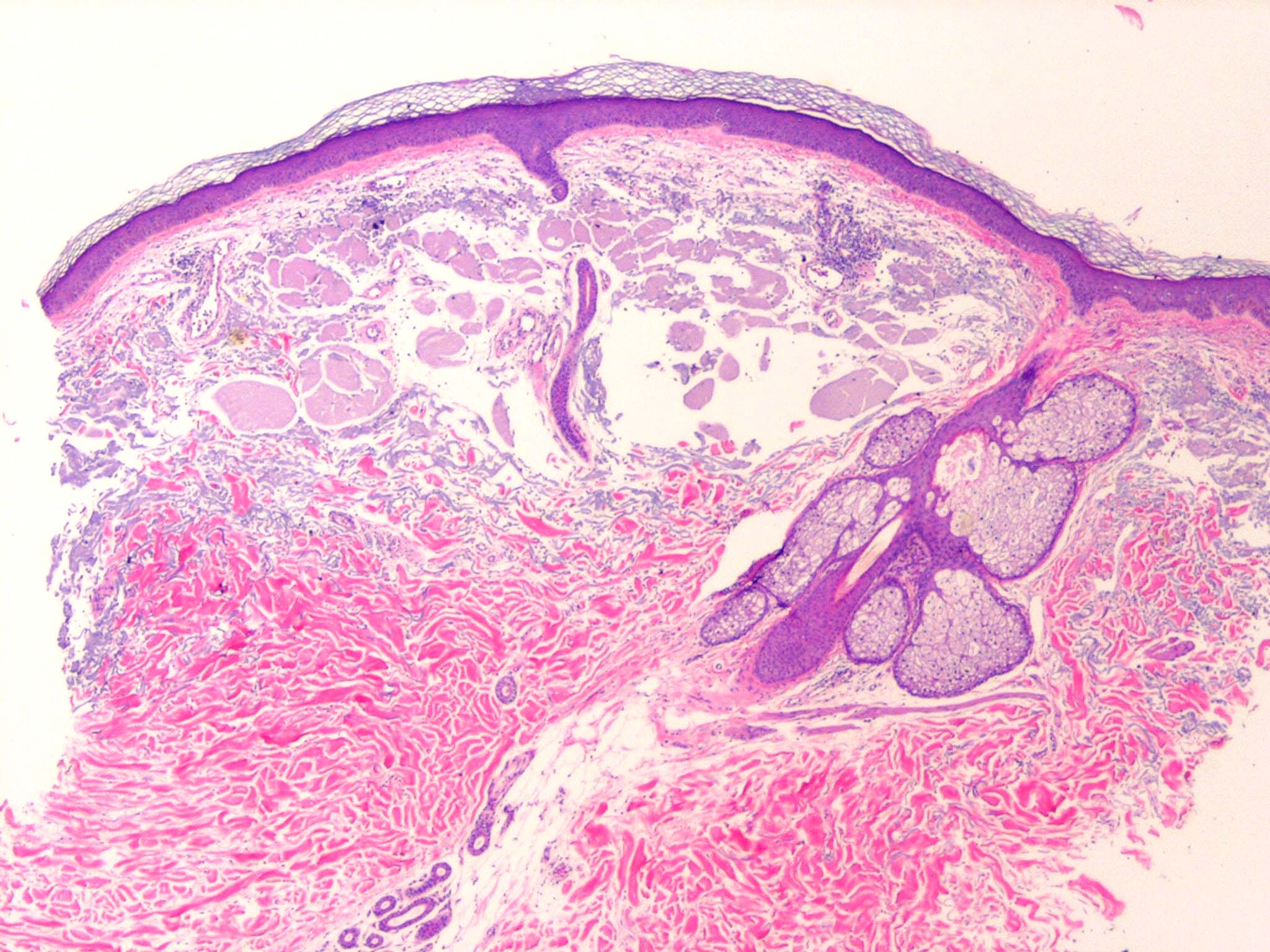
Colloid milium is a rare condition characterized by (1) the presence of multiple, dome-shaped, amber- or flesh-colored papules developing on light-exposed skin and (2) the observance of dermal colloid under light microscopy. The 4 variants are (1) an adult-onset type, (2) a nodular form (nodular colloid degeneration),1 (3) a juvenile form,2,3 and (4) a pigmented form, thought to be due to excess hydroquinone use for skin bleaching.4
Colloid milium is a degenerative condition linked to excessive sun exposure and possibly exposure to petroleum products and hydroquinone. The origin of the colloid deposition in the dermis is not certain, but it is thought to be due to degeneration of elastic fibers5,6 in the adult form and due to degeneration of UV-transformed keratinocytes in the juvenile form. Juvenile colloid milium is inherited.
Colloid milium is rare, but more than 100 case reports are present in the world literature. No known figures exist on prevalence.
Most cases of colloid milium persist with no natural resolution. Lesions reach their peak within 3 years, after which very few new papules occur.
Colloid milium is more common in fair-skinned individuals.
The adult form of colloid milium is more common in males.
The rare juvenile form of colloid milium occurs before puberty. Adult colloid milium is more common in elderly patients.
Papules develop gradually over the facial area and light-exposed sites. Patients with colloid milium are usually asymptomatic, but they may have transient itching in affected areas.
The physical findings in colloid milium are usually limited to the skin.
- Skin lesions of colloid milium: Amber, waxy, partially translucent, firm papules occur in crops, ranging from 1-5 mm in diameter. Gelatinous material can be expressed. In the nodular form, larger nodules (5-10 mm) or plaques develop. The underlying skin may be thickened, furrowed, and hyperpigmented. In the pigmented form, the papules are gray-black and confluent or clustered.
- Skin distribution of colloid milium lesions: The lesions occur on light-exposed skin, with the cheeks, periorbital area, nose, ears, and neck most frequently involved; however, lesions may also occur on the backs of the hands and forearms. Nodules arising on one side of the face and the ipsilateral forearm have been described in a taxi cab driver. Upper eyelid margin involvement alone has been reported.7 Juvenile colloid milium may be associated with ligneous conjunctivitis or ligneous periodontitis. Rarely, lesions occur in the oral cavity.
- The classic adult and nodular forms of colloid milium are believed to be due to excessive sun exposure, which appears to cause degeneration of elastin. Evidence to support this comes from the exposed site distribution and the tendency for colloid milium to occur in individuals with fair complexions and outdoor occupations.10,11
- The juvenile form of colloid milium is inherited, perhaps suggesting an inherited susceptibility to UV light. Autosomal recessive inheritance has been reported.
- An outbreak of colloid milium occurred in oil refinery workers in the tropics.13 A mechanic with occupational exposure to lubricating oils developed colloid milium over the backs of the hands.14 This may represent an interplay between light and petroleum constituents. Phenols have been suggested as causative agents.
- Prolonged use of hydroquinones has resulted in the development of the pigmented form of colloid milium, sometimes in association with ochronosis
-
Treatment
For colloid milium, no treatment is available that is entirely satisfactory.
Dermabrasion, cryotherapy, and diathermy have been tried with limited success. Advice about sunscreen use may also be helpful. Systemic ascorbic acid and exfoliating agents have also been tried with variable results. The Er:YAG laser may be more successful for colloid milium than dermabrasion