| Cutaneous B-cell lymphoma = اللمفوما الجلدية بائية الخلايا |
|
|
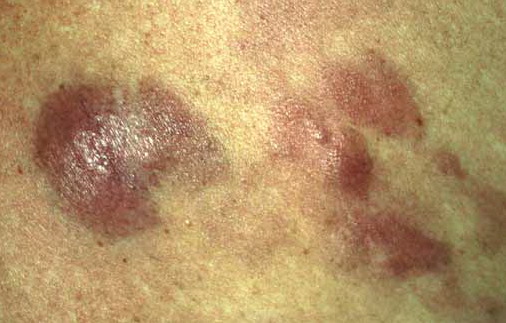
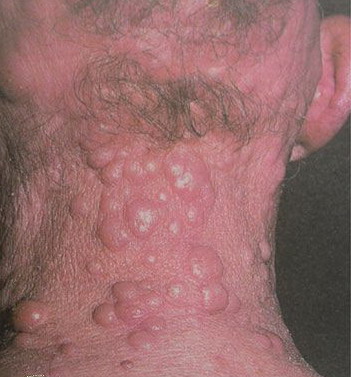
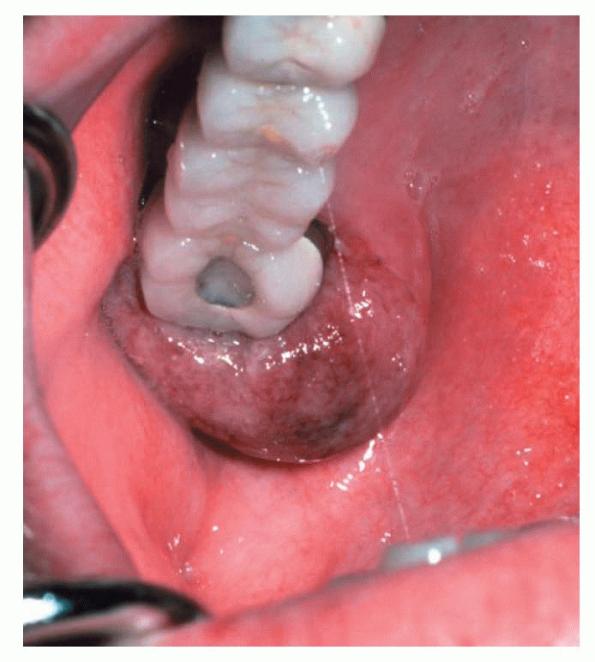
Cutaneous B-cell lymphoma Lymphoma is the most common blood cancer. The two main forms of lymphoma are Hodgkin lymphoma (HL) and non-Hodgkin lymphoma (NHL). Lymphoma occurs when lymphocytes, a type of white blood cell, grow abnormally. The body has two main types of lymphocytes that can develop into lymphomas: B-lymphocytes (B-cells) and T-lymphocytes (T-cells). Cancerous lymphocytes can travel to many parts of the body, including the lymph nodes, spleen, bone marrow, blood or other organs, and can accumulate to form tumors. B-cell lymphomas, which occur when B-lymphocyte cells become cancerous, account for 85 percent of all NHL cases in the United States. There are many different forms of B-cell lymphoma. Lymphomas that arise in organs or tissues outside of the lymphatic system are called extranodal lymphomas. When extranodal lymphomas originate in the skin (making up 18 percent of all extranodal lymphomas and 5 percent of all NHLs), and there is no evidence of disease outside of the skin, they are called primary cutaneous lymphomas. If B-cells are involved, they are called primary cutaneous B-cell lymphomas (CBCL). CBCLs are nearly always indolent (slow-growing). They may appear on the skin as a reddish rash, lump or nodule and may have a slightly raised and smooth appearance. The disease tends to recur on the skin, but will rarely develop into a systemic (throughout the body) lymphoma. Prognosis is usually very good, although relapse is common, with nearly 50 percent of those diagnosed with CBCL experiencing recurrence after an initial complete response to treatment. The disease affects men and women equally, and can affect any age group. Like all lymphomas, CBCL is an acquired disease and there are no known risk factors. The disease is not inherited nor is it contagious. Many of the same procedures used to diagnose and stage other types of lymphomas are used in CBCL, including a physical exam and history, blood tests, and a series of imaging tests such as CT (computerized axial tomography), MRI (magnetic resonance imaging) and/or PET (positron emission tomography) scans. A bone marrow biopsy may be necessary for more aggressive CBCLs. Types of Cutaneous B-Cell LymphomaPrimary cutaneous follicle center lymphoma is the most common B-cell lymphoma to develop as a primary tumor of the skin. These skin lymphomas develop slowly, over months or years, and may manifest as single or multiple tumors or nodules with a pink or reddish appearance. This disease usually appears on the head, neck or trunk of the body. Primary cutaneous marginal zone B-cell lymphoma is the second most common form of CBCL. This slow-growing lymphoma appears as pink or red lesions, nodules and/or tumors. It is most commonly found on the extremities, but can occur anywhere on the body. Primary cutaneous diffuse large B-cell lymphoma, leg-type is less common than other CBCLs, but is usually more aggressive (fast-growing), developing over weeks or months. This lymphoma usually appears as red or bluish-red lesions on the lower legs, although lesions can occur on any part of the body. The lesions frequently grow into large tumors that extend deep into the body. The lesions may become open sores and spread outside the skin more frequently than the slow-growing CBCLs. Primary cutaneous diffuse large B-cell lymphoma, other describes a group of very rare lymphomas, including intravascular large B-cell lymphoma, T-cell rich large B-cell lymphoma, plasmablastic lymphoma and anaplastic B-cell lymphoma. Although these lymphomas usually appear on the head, trunk and extremities, they are almost always cutaneous manifestations of systemic lymphomas and thus do not truly fit among the CBCLs. Treatment OptionsSelecting a treatment for a patient depends on the symptoms, the patient’s general health and stage of disease. Depending on the number of lesions present, primary cutaneous follicle center lymphoma and cutaneous marginal zone lymphoma may be treated locally with either radiation or surgery. Topical steroids or topical chemotherapy may also be used. Slow-growing CBCLs rarely transform into more aggressive types of lymphoma. For diseases that do transform, become widespread or become systemic, a variety of chemotherapy regimens may be used. Other therapies, such as rituximab (Rituxan) either alone or in combination with chemotherapy, or interferon may be recommended. There is no known best treatment strategy for the more aggressive types of CBCL such as cutaneous diffuse large B-cell lymphoma, leg type. For single tumors, radiation is often effective as are combinations of chemotherapy or radiation and chemotherapy given sequentially. All of these treatments usually put the disease in remission, however, relapse is common. Research is underway to test the most effective strategies for treating CBCLs. Treatments Under InvestigationThere are several treatments being tested in clinical trials for CBCL. It is critical to remember that today’s scientific research is continuously evolving. Treatment options may change as new treatments are discovered and current treatments are improved. Therefore, it is important that patients check with the Lymphoma Research Foundation or their physician for any treatment updates that may have recently emerged. Participating in Clinical TrialsClinical trials are crucial in identifying effective drugs and determining optimal doses for lymphoma patients. Patients interested in participating in a clinical trial should talk to their physician. Contact the Lymphoma Research Foundation’s Helpline for an individualized clinical trial search by calling (800) 500-9976 or emailing This e-mail address is being protected from spambots. You need JavaScript enabled to view it . Follow UpOnce treatment is completed, a follow-up care plan should be created by the patient’s physician. The plan should provide a treatment summary, which includes information such as age and date of diagnosis, staging, the types of treatment administered and response to treatment. The plan should also indicate the type and frequency of medical tests that a survivor should routinely undergo over their lifespan. Lymphoma survivors should receive regular medical exams from a physician who is familiar with their medical history as well as the treatments they have received. Survivors and their caregivers are encouraged to keep copies of all medical records and test results as well as information on the types, amounts and duration of all treatments received. This documentation will be important for keeping track of any effects resulting from treatment or potential disease recurrences. |