
RUBELLA
Epidemiology
Rubella virus has a worldwide distribution with outbreaks occurring most frequently in late winter and early spring months. School-aged children, adolescents, and young adults most often develop the disease. Epidemics occasionally occur in developing countries, especially where vaccines are unavailable.
RUBELLA AT A GLANCE
· German measles, 3-day measles.
· Epidemic disease; worldwide distribution.
· Short prodrome; rash of 2- to 3-day duration.
· Enlargement of cervical, suboccipital, and postauricular glands.
· High risk of fetal malformations with congenital infection (microcephaly, congenital heart disease, deafness), particularly in the first trimester.
Since introduction of the rubella vaccine in the United States in 1969, the incidences of rubella and congenital rubella syndrome have drastically declined with no widespread epidemics occurring in the United States. Occasional outbreaks have largely been attributed to failure to vaccinate susceptible individuals.
Etiology and Pathogenesis
Rubella is an enveloped RNA virus in the Togaviridae family. The virus is spread through direct or droplet contact from nasopharyngeal secretions. Infected individuals shed virus for 5 to 7 days before and 14 days after onset of disease, with viremia unlikely after the rash occurs. In most individuals, infection leads to lifelong immunity.
Congenital rubella occurs when a nonimmunized, susceptible, pregnant woman is exposed to the virus. Transplacental infection of the fetus occurs during the viremic stage. The risk is greatest to a fetus exposed to the virus in the first trimester. Congenitally infected infants may shed the virus through urine, blood, and nasopharyngeal secretions for up to 12 months after birth, thus being a potential source of viral exposure to other susceptible individuals.
Clinical Findings
HISTORY
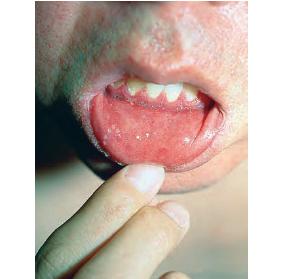
Primary rubella infection is typically a mild, sub-clinical disease, particularly in adults. The prodrome is characterized by low-grade fever, myalgias, headache, conjunctivitis, rhinitis, cough, sore throat, and lymphadenopathy; symptoms that may last up to 4 days and often resolve with appearance of rash. Up to 50 percent of children with primary rubella infection may have a sub-clinical infection or present only with lymphadenopathy or rash (no prodrome). Conversely, older adults may have more severe and persistent prodromal symptoms that may make distinction from rubeola difficult in some situations. The presence of Koplik spots in the mouth favors rubeola. As the prodrome resolves and the rash begins to appear, some patients develop an enanthem consisting of tiny red macules on the soft palate and uvula (Forschheimer spots). This enanthem is not diagnostic for rubella.
CUTANEOUS LESIONS
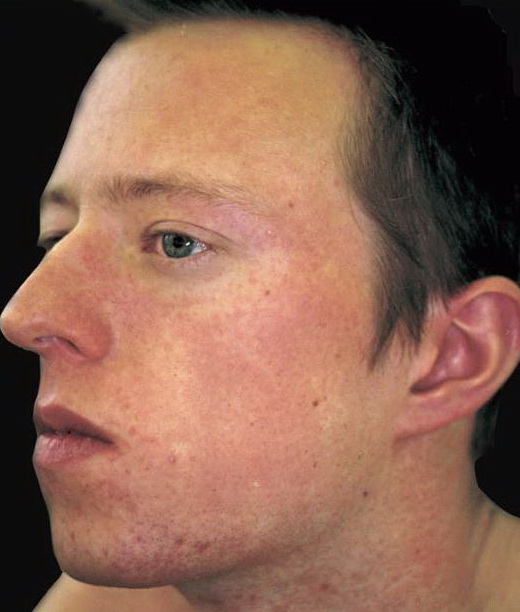
The exanthem, occurring 14 to 17 days after exposure, is characterized by pruritic pink to red macules and papules that begin on the face, quickly progressing to involve neck, trunk, and extremities (Fig. 192-4 and At a Glance image). Lesions on the trunk may coalesce, whereas those on the extremities often remain more discrete. The rash usually begins to disappear in 2 to 3 days, unlike rubeola, which can be more persistent and clears the head and neck first. Desquamation may follow resolution of the rash.
RELATED PHYSICAL FINDINGS
Lymphadenopathy is usually most severe in the posterior cervical, suboccipital, and postauricular lymph nodes and is noted up to 7 days before the rash appears.27 Enlargement of the nodes may persist for several weeks.
Adults, particularly women (up to 70 percent), may develop arthritis with rubella infection.27 Both small and large joints may be affected. Joint symptoms often first appear as the rash fades and can last several weeks. In some individuals, the symptoms may become persistent or recurrent. Joint swelling may progress to form a joint effusion.
Laboratory Tests
Serum complete blood cell count usually shows leukopenia with relative neutropenia. Increased numbers of atypical lymphocytes or abundant plasma cells may be noted as well. Patients with meningeal involvement have lymphocytes in the cerebrospinal fluid (CSF). Viral culture (nose, throat, blood, urine, CSF, synovial fluid) is sensitive but often difficult due to the unstable nature of the virus. Diagnosis is typically made using serology to detect rubella-specific IgM antibody (up to 8 weeks after infection) or to document a fourfold rise in antibody titer in acute and convalescentphase serum. Hemagglutination-inhibition, complement fixation, immunofluorescence assay, and ELISA are some of the methods used to detect antibodies. As with measles, rubella cases should be reported to local health departments.
Congenital Rubella Syndrome
Women who are infected with rubella during pregnancy may only exhibit minor clinical symptoms. The effects, however, of rubella infection on the fetus can be profound, with the greatest risk of fetal malformation in the early stages of pregnancy. Up to 85 percent of fetuses exposed to rubella within the first 4 weeks develop serious sequelae such as: microcephaly with mental retardation, congenital heart disease (ventricular septal defect, patent ductus arteriosus), sensorineural deafness, cataracts, low birth weight and fetal death.
Diagnosis of congenital rubella infection is obtained by isolating rubella virus in the throat, urine, or CSF of the affected neonate. Serologic testing is not as sensitive but is easily available for confirmatory testing.
Differential Diagnosis of Rubella
Most Likely
· Drug hypersensitivity reaction
· Rubeola (measles)
Consider
· Other viral infection (enterovirus, adenovirus, parvovirus, human herpesvirus-6)
Always Rule Out
· Streptococcal scarlet fever
Complications
Rarely, rubella infection may lead to encephalitis (1 in 6000 cases), with mortality rates varying from 0 percent to 50 percent.Other rare complications include: peripheral neuritis, optic neuritis, myocarditis, pericarditis, hepatitis, orchitis, and hemolytic anemia. Transient thrombocytopenia has been described in 1 in 3000 children (usually girls); first appearing within days of rash onset and lasting days to months. Recently, a case of rubella-associated hemophagocytic syndrome in an infant was described.
Prognosis and Clinical Course
Rubella is typically a self-limited disease. Infants who have congenital rubella are infectious until viral shedding from the nasopharynx and urinary tract ends. The majority of infants (85 percent) infected in utero excrete virus in the first month of life; 1 percent to 3 percent continue to excrete virus in the second year of life. Pregnant women caring for these infants are at risk for developing rubella. Clinical course depends on how severely affected the fetus is from intrauterine infection.
Treatment
Treatment of primary, uncomplicated rubella is supportive. In nonpregnant individuals, rubella vaccine administration within 3 days of exposure may theoretically prevent illness, though this is yet to be proven.27 Immune globulin is not routinely recommended as post-exposure prophylaxis of rubella-susceptible pregnant women. Limited data indicate that intramuscular immune globulin (0.55 mL/kg) may decrease clinically apparent infection from 87 percent to 18
percent if given to an exposed, susceptible pregnant woman. However, absence of clinical signs after administration of immune globulin does not assure that congenital infection did not occur.
Neonates with congenital rubella syndrome require supportive care as well as appropriate attention to significant health issues. These infants are contagious and should be isolated to prevent transmission to susceptible individuals. Contact isolation is recommended for these infants until they are at least 12 months old or if repeated cultures are negative after 3 months of age.
Prevention (Immunizations)
Rubella vaccine is typically administered as part of a three-fold vaccine (MMR) at 12 to 15 months of age and again at 4 to 6 years of age. Seroconversion after a single dose of MMR vaccine occurs in 95 percent individuals.It is imperative that individuals at risk for rubella infection are immunized, such as health care workers, military recruits, college students, and recent immigrants.27 Individuals are considered immune to rubella if they have documented vaccination with a live MMR on or after their first birthday, serologic evidence of rubella immunity, or were born after 1957 (except women of childbearing age).
Potential adverse reactions to rubella vaccine occur in susceptible individuals and include: fever, morbilliform rash, lymphadenopathy, and arthralgia.
Pregnant woman should not be immunized with rubella to minimize risk to the fetus. Any woman receiving the rubella vaccine should not become pregnant for 28 days. Infants of vaccinated breast-feeding mothers may become infected with rubella via breast milk. Typically they develop a mild erythematous exanthem of macules and papules with no serious effects. As rubella infection confers lifelong immunity, a woman who is re-exposed during pregnancy has a low risk of having her fetus contract congenital rubella. Concern about possible infection can be addressed by looking for IgM antibodies in fetal serum (cordocentesis).