Hand Foot Mouth
Disease
EPIDEMIOLOGY
HFMD is a disease with worldwide distribution that is usually self-limited. There is a slight male predominance. Children less then 10 years of age are most frequently affected and infected adults rarely show signs of infection. Similar to exanthems caused by other enteroviruses, HFMD occurs more during summer and fall in temperate climates and throughout the year in the tropics. Outbreaks may be sporadic or in epidemics. The largest recorded epidemic was in Taiwan in 1998. This epidemic affected over 120,000 people and caused 78 deaths.
Transmission is via fecal-oral route and, less commonly, respiratory inhalation. There is a high transmission rate among household contacts as has been documented with studies of epidemics.
Once inhaled or ingested, virus replication ensues in the oropharynx and/or gastrointestinal tract with subsequent viremia. The incubation period of HFMD is believed to be short, lasting 3 to 6 days, with viral shedding lasting up to 5 weeks.263
HAND-FOOT-MOUTH DISEASE AT
AGLANCE
· Viral exanthem seen mostly commonly in children in summer and fall.
· Erosions in the mouth and papulovesicles on the palms and soles.
· Caused by enteroviruses including coxsackievirus A16 and enterovirus 71.
· Self-resolving without serious sequelae in the majority of cases but may have serious complications when caused by enterovirus 71
ETIOLOGYANDPATHOGENESIS
HFMD is caused by a number of non-polio enteroviruses, including coxsackieviruses A5, A7, A9, A10, A16, B1, B2, B3, B5, echoviruses, and other enteroviruses. The most common causes are coxsackie A16 and enterovirus 71. Enteroviruses belong to the Picornaviridae family, which are single-stranded RNA viruses.
CLINICAL FINDINGS
History.
After an incubation phase of 3 to 6 days, affected individuals may complain of a low-grade fever, malaise, abdominal pain, and upper respiratory tract symptoms.
Cutaneous Lesions.
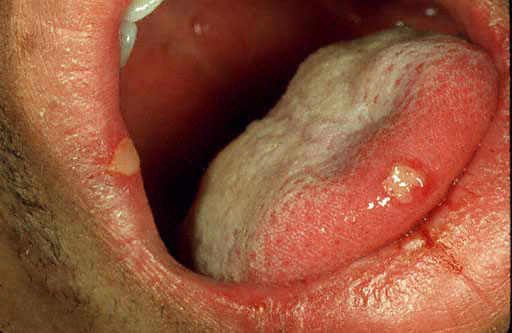
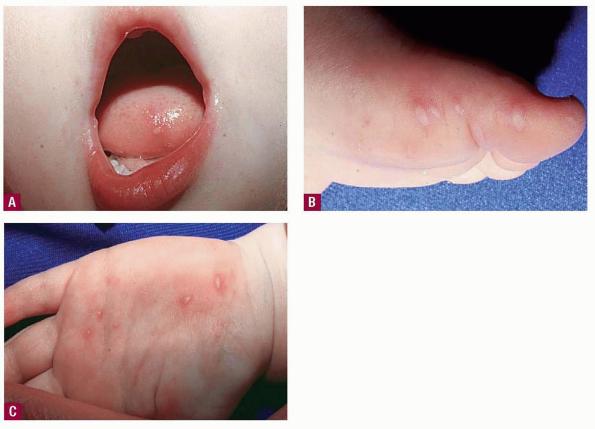
Nearly all cases of HFMD have painful oral lesions. These are generally few in number and are found on the tongue , buccal mucosa, hard palate, and, less frequently, the oropharynx. The lesions start as bright pink macules and papules that progress to vesicles with surrounding erythema. These quickly erode and form yellow to gray erosions surrounded by an erythematous halo. The time between vesicle and erosion is short, and most patients have erosions by the time they visit their physician.
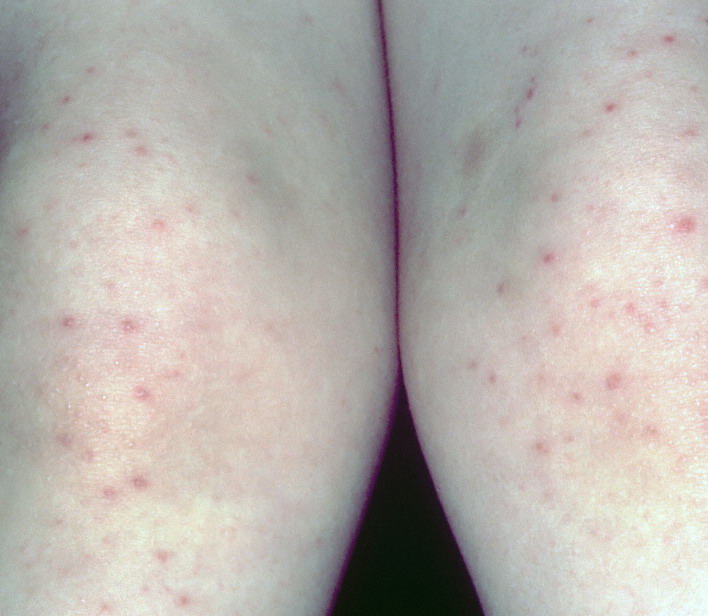
Cutaneous peripheral lesions are present in two-thirds of patients and appear soon after the oral lesions. The lesions are most common on the palms, soles , sides of hands and feet, buttocks and, occasionally, external genitalia, and on the face and legs. They evolve similarly to the oral lesions, starting as red macules that become clear oval, elliptical (football-shaped), or triangular vesicles with surrounding red halos The number of lesions ranges from few to numerous. After crusting, they heal in 7 to 10 days.
Related Physical Findings.
HFMD usually begins with a non-specific prodrome, including low-grade fever [38°C to 39°C (100.4°F to 102.2°F)] that lasts 1 to 2 days, malaise, and, occasionally, abdominal pain or upper respiratory tract symptoms. Sore throat or sore mouth is common and may lead to poor oral intake and dehydration. Cervical and submandibular lymphadenopathy may be present.
LABORATORY TESTS
No laboratory tests are indicated. If an epidemic is suspected, stool and throat cultures may be helpful in determining the strain and, therefore, possible complications.
SPECIAL TESTS
Historically, enteroviral infection was verified by viral culture, which lacked sensitivity, and suckling mouse inoculation, which detected neutralizing antibodies. Recently, PCR has been found to be very effective in detection and identification of enterovirus serotypes. PCR may be very useful if it becomes widely available.
DIFFERENTIAL DIAGNOSIS
COMPLICATIONS
Patients rarely experience complications from HFMD. One rare complication, called eczema coxsackium, occurs in individuals with eczema. These patients develop disseminated cutaneous viral infection similar to that seen in eczema herpeticum. The most common serious complication associated with HFMD is aseptic meningitis. Aseptic meningitis is rarely life-threatening, and patients do not develop permanent sequelae. Epidemics in Taiwan of enterovirus 71 have resulted in severe disease with encephalitis, encephalomyelitis, polio-like syndromes, myocarditis, pulmonary edema, pulmonary hemorrhage, and death. Serious complications are less frequent in cases associated with coxsackievirus A16 than with enterovirus 71.
Differential Diagnosis of Hand-
Foot-Mouth Disease
Most Likely
· Herpangina
Consider
· Varicella
· Aphthous stomatitis
· Drug eruption
· Erythema multiforme
Always Rule Out
· Herpes gingivostomatitis
PROGNOSIS AND CLINICAL COURSE
HFMD is usually a benign, self-limited illness that resolves within 7 to 10 days. Occasionally, cases associated with more prolonged fever, systemic symptoms, diarrhea, and joint pains have been reported.
PREVENTION
During epidemics, public health measures should be instituted to decrease morbidity. Measures such as universal precautions, dissuading attendance at childcare centers or kindergarten, and isolating affected individuals have been suggested.