





















Neurotic Excoriations
Patients consciously create neurotic excoriations by repetitive scratching. Neurotic excoriations should be distinguished from dermatitis artefacta, in which patients create lesions for secondary gain. Neurotic excoriations can be initiated by some minor skin pathology, such as an insect bite, folliculitis, or acne, but it can also be independent of any pathology. Because no significant underlying pathology is present in the skin, neurotic excoriations are really a psychologic process with dermatologic manifestations. Many doctors lack an extensive understanding of neurotic excoriations and its treatment.1
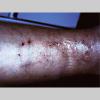
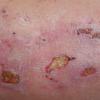
Because patients create neurotic excoriations, the lesions have the quality of "an outside job," that is, clean, linear erosions, crusts, and scars that can be hypopigmented or hyperpigmented. The erosions and scars of neurotic excoriations often have irregular borders and are usually similar in size and shape. They occur on areas that the patient can scratch, particularly the extensor surfaces of the extremities, the face, and the upper part of the back. The distribution is bilateral and symmetric.
The manifestations of neurotic excoriations vary widely from unconscious picking at the skin to uncontrollable picking at lesions to remove imaginary foreign bodies. Picking is usually episodic and irregular, but it can be constant. The picking can have the quality of a ritual and may take place in a state of dissociation.
In 2006, Shah and Fried2 reported that neurotic excoriations are among the most common factitial skin diseases observed in children. They further noted that factitial skin disease is less common in children and can often be linked to comorbid psychiatric diagnoses or a psychosocial stressor that can be identified.
Pathophysiology
Neurotic excoriations are due either to an underlying psychopathology or to the formation of habit. As such, its pathophysiology is poorly understood.
History
Patients give a history of picking, digging, or scraping their skin. Sometimes, an inciting incident is the cause, and, sometimes, no inciting incident is present. Patients might note that they do not scratch themselves consciously; rather, they pick and then notice that they are picking. Cyr and Dreher4 have an excellent summary of neurotic excoriations and their historical and clinical findings and manifestations.
Patients can have a psychiatric history that includes depression, obsessive-compulsive disorder, and anxiety. Most patients do not have any particular psychopathology; however, psychiatric diagnoses to be considered include the following:
- Depression
- Trichotillomania
- Anxiety
- Tic disorder
- Obsessive-compulsive disorder
- Body dysmorphic disorder
- Somatoform disorders (eg, facial dermatitis, somatization, hypochondriasis)
- Borderline personality disorder (self-mutilation)
- Delusions of parasitosis (may be part of a larger diagnostic group, such as schizophrenia)
Patients pick at areas until they can pull material from the skin. This may be referred to as "pulling a thread from the skin."Setyadi et al5 noted that trigeminal trophic syndrome can result in nasal ulcerations (the nasal ala and paranasal locations), most commonly manifesting in older women following therapy for trigeminal neuralgia.Young women who pick at their faces may have a history of mild acne. Such cases are referred to as acne excoriée. This condition is not discussed in this article. The erosions can heal slowly because of recurrent picking.Asking the patient what came first the lesion or the urge to itch is useful. On close questioning, most patients say that they scratched their skin and then saw a lesion. The lesions of neurotic excoriations have a component of an itch-scratch cycle, whereby the urge to scratch generates an even greater urge to scratch.Because a variety of conditions can cause itching and then lesions, these must be excluded or, at least, not considered as likely to firmly make a diagnosis of neurotic excoriation. These conditions include the following:
- Scabies
- Dermatitis herpetiformis
- Renal disease
- Cocaine use
- Opiate use
- Medication reactions
- Multiple sclerosis
- Hepatic disease
- Lymphoma
- Pregnancy
- Internal cancers
- Uremia
- Carcinoid
- Delirium
- Polycythemia vera
- Diabetes mellitus
- Hypothyroidism
- Iron deficiency anemia
- Hyperthyroidism
- Xerosis
- Urticaria
- Intestinal parasitosis
Myeloma can be reported.Patients may report headache or menstrual disorders.As reported by Shenefelt in 2004,6 hypnotic suggestion successfully alleviated the behavioral picking aspect of acne excoriée des juenes filles in a pregnant woman who had been picking at the acne lesions on her face for 15 years. Acne excoriée is a subset of psychogenic or neurotic excoriation. Conventional topical antibiotic treatment was used to treat the acne. Compared with other treatments for uncomplicated acne excoriée, hypnosis is relatively brief and cost-effective and is nontoxic in pregnancy.
Physical
Often, right-handed persons tend to pick at their left side and left-handed people pick at their right side. The erosions and scars tend to have angulated borders. The quantity of erosions and scars is variable. Several lesions to hundreds of lesions can be present. Erosions, crusts, and scars are only located where the patient can pick. Lesions can be crusted or noncrusted
Erosions can vary in morphology and can sometimes evolve into frank ulcers. Dug-out erosions or ulcers, crusted erosions, and ulcers can be present. Sometimes, erythema and scars are present around the erosions and the ulcers.
In dermatitis artefacta, the patient creates skin lesions to satisfy an internal psychological need, usually a need to be taken care of. The clinical presentation is characteristic, and it differs from that of neurotic excoriations, delusional disorders, malingering, and Munchausen syndrome. Munchausen syndrome by proxy is a form of dermatitis artefacta.
Except when the lesions mimic another disease, those that do not conform to descriptions of known dermatoses are shrouded in mystery, appearing fully formed on accessible skin, within the context of a characteristic psychological constellation. The patient is friendly but bewildered, and relatives may be angry and frustrated.
Because of lack of diagnostic stringency, quoted female-to-male ratios range from 3-20:1, with the highest incidence of onset in late adolescence to early adult life. Most patients have a personality disorder; borderline features are common.
The patient's denial of psychic distress and the possible negative feelings aroused in health care personnel make management difficult.
Setting limits for the protection of both the physician and patient; creating an accepting, empathic, and nonjudgmental environment; and closely supervising symptomatic dermatologic care permit the development of a therapeutic relationship in which psychological issues may be gradually introduced, which may occasionally permit referral to a psychiatrist. Issues of etiology should be sidestepped because confrontation is counter-productive.
If the patient refuses referral to a psychiatrist, psychotropic drug therapy prescribed by dermatologists is helpful and appropriate. The upper dose range of selective serotonin reuptake inhibitors (SSRIs) or low-dose atypical antipsychotic agents may be effective.
Except in mild transient cases triggered by an immediate stress, the prognosis for cure is poor. The condition tends to wax and wane with the circumstances of the patient's life.
Lesions can be kept to a minimum, the patient can be protected from unnecessary and intrusive studies, and society can be protected from escalating and unnecessary expenditure of medical resources if, rather than discharging the patient, the dermatologist continues to see the patient on an ongoing basis for supervision and support, regardless of whether lesions are present.
Research studies are necessary to more accurately document the expectable cause, treatment outcome, and prognosis for this group of patients.
Causes
The causes of neurotic excoriations are manifold and can relate to picking as a means of resolving stress or some underlying psychopathology.7 Some believe neurotic excoriations are a physical manifestation of obsessive-compulsive disorder.
Laboratory Studies
To rule out systemic disease, perform the following tests:
- Complete blood cell count with differential
- Chemistry profile
- Determination of thyrotropin levels
- Fasting plasma glucose level
Medical Care
In 2005, Krishnan and Koo8 reported that the pathology of the opioid neurotransmitter system and the central nervous system is the neurological basis for neurotic excoriations and thus psychiatric medications that can normalize nervous system pathology can abate neurotic excoriations.
In the treatment of neurotic excoriations, studies have shown that the serotonergic effect of selective serotonin reuptake inhibitors (SSRIs) produce an antipruritic effect.9 The relief of pruritus is unrelated to changes in the patient's mood and happens faster than would be expected for antidepressant effects.
For its sedating and antipsychotic effects, doxepin (10-25 mg PO qhs) is a useful medication in treating neurotic excoriations.
Dereli et al10 found that gabapentin is a useful treatment for recalcitrant chronic prurigo nodularis.
Surgical Care
Physical barriers such as an Unna sleeve can be an effective treatment for neurotic excoriations.11
























