Staphylococcal
Ecthyma.
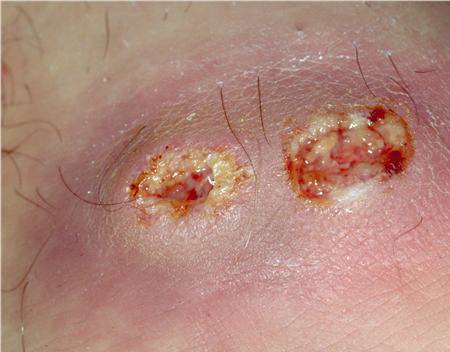
Ecthyma is a cutaneous pyoderma characterized by thickly crusted erosions or ulcerations. Ecthyma is usually a consequence of neglected impetigo and classically evolves in impetigo occluded by footwear and clothing. It thus is a lesion typically occurring in the homeless and soldiers in combat on maneuver in a humid and hot climate. S. aureus and/or group A streptococcus can be isolated on culture. Untreated staphylococcal or streptococcal impetigo can extend more deeply, penetrating the epidermis, producing a shallow crusted ulcer . Ecthymatous lesions can evolve from a primary pyoderma or within a pre-existing dermatosis or site of trauma. Ecthyma gangrenosum is a cutaneous ulcer caused by P. aeruginosa and resembles staphylococcal or streptococcal ecthyma .
Differential Diagnosis of Bullous Impetigo
Consider
· Contact dermatitis
· Bullous insect bites
· Bullous tinea
· Bullous fixed drug reaction
· Bullous drug eruption
· SSSS
· Thermal burns
· Pemphigus vulgaris
· Bullous pemphigoid
· Erythema multiforme
· Dermatitis herpetiformis
Always Rule Out
· Herpes simplex
· Varicella
· Bullous tinea
· Bullous fixed drug reaction
· Bullous drug eruption
· SSSS
SSSS = staphylococcal scalded-skin syndrome. Note: Any of these disorders may occur primarily and become secondarily impetiginized with Staphylococcus aureus or group A streptococcus.
Ecthyma occurs most commonly on the lower extremities of children, or neglected elderly patients, or individuals with diabetes. Poor hygiene and neglect are key elements in pathogenesis. Multiple ecthymatous ulcers on the ankle and dorsum of the foot were the most common pyodermas seen during wartime in tropical climates.
Treatments for Impetigo
|
|
TOPICAL
|
|
SYSTEMIC
|
|
|
First line
|
Mupirocin
|
bid
|
Dicloxacillin
|
250-500 mg PO qid for 5-7 days
|
|
Fusidic acid (not available in United States)
|
bid
|
Amoxicillin plus clavulanic acid; cephalexin
|
25 mg/kg tid; 250-500 mg qid
|
|
|
Second line (penicillin allergy)
|
|
|
Azithromycin
|
500 mg × 1, then 250 mg daily for 4 days
|
|
|
|
Clindamycin
|
15 mg/kg/day tid
|
|
|
|
Erythromycin
|
250-500 mg PO qid for 5-7 days
|
The ulcer has a “punched out” appearance when the dirty grayish-yellow crust and purulent material are débrided. The margin of the ulcer is indurated, raised, and violaceous , and the granulating base extends deeply into the dermis. Untreated ecthymatous lesions enlarge over weeks to months to a diameter of 2 to 3 cm or more.
The lesions are slow to heal, requiring several weeks of antibiotic treatment for resolution. Problems of spread by autoinoculation or by insect vectors and of post-streptococcal sequela (glomerulonephritis) are the same as with impetigo.
Management of ecthyma is the same as for staphylococcal impetigo .