|
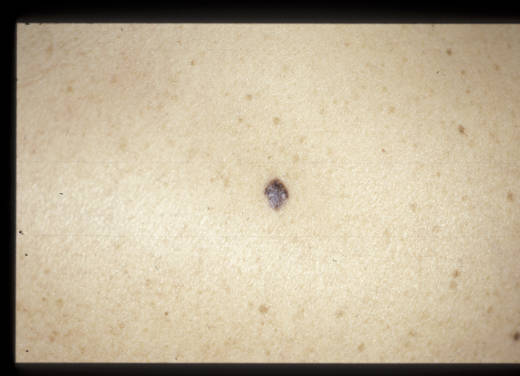
Carcinome basocellulaire pigmenté= الورم القاعدي الخلايا المصطبغ |
 |
 |
 |
Basal cell carcinoma
Basal cell carcinoma (BCC) is the most common skin cancer in humans. Basal cell skin cancer tumors typically appear on sun-exposed skin, are slow growing, and rarely metastasize (0.028-0.55%). Neglected tumors can continue to grow and lead to significant local destruction and even disfigurement
Basal cell carcinoma is a nonmelanocytic skin cancer (ie, an epithelial tumor) that arises from basal cells, small round cells found in the lower layer of the epidermis. Tumor size can vary from a few millimeters to several centimeters in diameter. Basal cells invade the dermis but seldom invade other parts of the body.
Basal cell carcinomas have a typical body distribution: 70% on head (most frequently on face1 ), 25% on trunk,2 and 5% on penis,3 vulva,4,5 or perianal skin. Very rarely, other organs are affected.6 Basal cell carcinoma has a high frequency in older men who have a long history of unprotected exposure to ultraviolet (UV) light. Basal cell carcinoma can develop on unexposed areas; cases of basal cell carcinoma of the prostate have been reported. In a few patients, the contributing factors are contact with arsenic,5,7 tar, coal, paraffin,8 certain types of industrial oil, radiation exposure, scars (ie, burn complications),9 xeroderma pigmentosum,10 vaccinations, or even tattoos.
The DNA of certain genes is often damaged in patients with basal cell carcinoma; therefore, inheritance may be a factor. Most DNA alterations result from damage caused by exposure to sunlight.
Pathophysiology
Although the exact etiology of basal cell carcinoma is unknown, a well-established relationship exists between basal cell carcinoma and the pilosebaceous unit, as tumors are most often discovered on hair-bearing areas. Tumors are currently believed to arise from pluripotent cells (which have the capacity to form hair), sebaceous glands, and apocrine glands. Tumors usually arise from the epidermis or the outer root sheath of a hair follicle.
Patient geographical location affects the risk of developing skin cancer. Basal cell carcinoma is related to lifetime exposure to UV radiation and a history of sunburn. The damaging effects of the sun are cumulative. The skin can repair superficial damage, but the underlying damage remains, including DNA damage. The damage worsens with each successive sun exposure, causing a lifetime progression.11 This damage reduces the ability of DNA to control cell growth and division and, in some situations, this progression results in cancer.
Almost all forms of basal cell carcinoma have mutations in the gene encoding the Hedgehog (Hh) receptor molecule, a signaling pathway playing a pivotal role in cell differentiation. At least 3 forms of this protein are known: sonic HH (SHH), Indian HH (IHH), and desert HH (DHH)
History
Patients often report a slowly enlarging lesion that does not heal and that bleeds when traumatized. As tumors most commonly occur on the face, patients often give a history of an acne bump that occasionally bleeds.
People who sunburn are more likely to develop skin cancer than those who do not; however, sunlight damages the skin with or without sunburn. Consider basal cell carcinoma in any patient with a history of a sore or skin anomaly that does not heal within 3-4 weeks and occurs on sun-exposed skin, especially if it is dimpled in the middle. These tumors may take many months or years to reach even 1 cm in diameter.
- Patients often have a history of chronic sun exposure.
- Recreational sun exposure (eg, sunbathing, outdoor sports, fishing, boating)
- Occupational sun exposure (eg, farming, construction)
- Occasionally, patients have a history of exposure to ionizing radiation. X-ray therapy for acne was commonly used until 1950.
- Occasionally, patients have a history of arsenic intake; arsenic is found in well water in some parts of the United States.
Physical
Basal cell carcinoma occurs mostly on the face, head (scalp included), neck, and hands.14 It rarely develops on the palms and soles. Basal cell carcinoma usually appears as a flat, firm, pale area that is small, raised, pink or red, translucent, shiny, and waxy, and the area may bleed following minor injury. Basal cell carcinomas may have one or more visible and irregular blood vessels, an ulcerative area in the center that often is pigmented, and black-blue or brown areas. Large basal cell carcinomas may have oozing or crusted areas. The lesion grows slowly, is not painful, and does not itch.
Clinical presentation of basal cell carcinoma varies by type.
- Nodular basal cell carcinoma
- Nodular basal cell carcinoma is the most common type of basal cell carcinoma and usually presents as a round, pearly, flesh-colored papule with telangiectases. As it enlarges, it frequently ulcerates centrally, leaving a raised, pearly border with telangiectases, which aids in making the diagnosis.
- Most tumors are observed on the face, although the trunk and extremities also are affected.
- Cystic basal cell carcinoma
- An uncommon variant of nodular basal cell carcinoma, cystic basal cell carcinoma is often indistinguishable from nodular basal cell carcinoma clinically, although it might have a polypoid appearance.
- Typically, a bluish-gray cyst-like lesion is observed. The cystic center of these tumors is filled with clear mucin that has a gelatin-like consistency.
- Pigmented basal cell carcinoma
- Pigmented basal cell carcinoma is an uncommon variant of nodular basal cell carcinoma that has brown-black macules in some or all areas, often making it difficult to differentiate from melanoma.
- Typically, some areas of these tumors do not retain pigment; pearly, raised borders with telangiectases that are typical of a nodular basal cell carcinoma can be observed. This aids clinically in differentiating this tumor from a melanoma.
- Morpheaform (sclerosing) basal cell carcinoma
- Morpheaform basal cell carcinoma is an uncommon variant in which tumor cells induce a proliferation of fibroblasts within the dermis and an increased collagen deposition (sclerosis) that clinically resembles a scar. The tumor appears as a white or yellow, waxy, sclerotic plaque that rarely ulcerates. The morpheaform subtype is the most difficult subtype to diagnose.
- Because the tumor infiltrates in thin strands between collagen fibers, treatment is difficult, and the clinical margins are difficult to distinguish. Mohs micrographic surgery is the treatment of choice for this type of basal cell carcinoma.
- Superficial basal cell carcinoma
- Superficial basal cell carcinoma is often multiple, most often developing on the upper trunk or shoulders. It grows slowly and appears clinically as an erythematous, well-circumscribed patch or plaque, often with a whitish scale. Occasionally, minute eschars may appear within the patch or plaque.
- The tumor appears multicentric, with areas of clinically normal skin intervening among clinically involved areas.
- Mental retardation
- Congenital agenesis of the corpus callosum and medulloblastoma
- Odontogenic jaw cysts
- Bifid ribs and pectus excavatum
- Absent or undescended testes
- Mesenteric lymphatic cysts
- Palmar and plantar pits
- Ectopic calcification (particularly of the falx cerebri)
- Ocular and skeletal abnormalities (eg, hypertelorism, shortening of the fourth and fifth metacarpals)
- Exposure to sunlight: Sunlight is the most frequent association, and risk is associated with the amount and nature of accumulated sun exposure over a lifetime, especially during childhood. UVB, 290-320 nm, which causes sunburn, is believed to play a greater role in the development of basal cell carcinoma than UVA.18
- Gene mutations: Recent studies demonstrate a high incidence of p53 gene mutations in basal cell carcinoma. Researchers speculate that UV sunlight may play an important role in the genesis of this mutation; however, genetic involvement has been demonstrated on chromosome 9 only in patients with familial basal cell nevus syndrome (Gorlin syndrome). Such mutation involves the PTCH gene, a tumor suppressor gene.
- Exposure to artificial ultraviolet light (eg, tanning booths, ultraviolet light therapy)
- Ionizing radiation exposure (eg, x-ray therapy for acne)
- Arsenic exposure through ingestion: Arsenic was used as a medicinal agent, predominantly Fowler's solution of potassium arsenite, which was used to treat many disorders, including asthma and psoriasis. A contaminated water source has been the most common source of arsenic ingestion.
- Immunosuppression: A modest increase in the lifetime risk of basal cell carcinoma has been noted in chronically immunosuppressed patients, such as recipients of organ or stem cell transplants.
- Xeroderma pigmentosum: This autosomal recessive disease results in the inability to repair UV-induced DNA damage. Pigmentary changes are seen early in life followed by the development of basal cell carcinoma, squamous cell carcinoma, and malignant melanoma. Other features include corneal opacities, eventual blindness, and neurological deficits.
- Nevoid basal cell carcinoma syndrome (basal cell nevus syndrome, Gorlin syndrome): In addition to basal cell carcinoma, this autosomal dominant disorder can result in the early formation of multiple odontogenic keratocysts, palmoplantar pitting, intracranial calcification, and rib anomalies. Various tumors such as medulloblastomas, meningioma, fetal rhabdomyoma, and ameloblastoma also can occur.19
- Bazex syndrome: Features include follicular atrophoderma ("ice pick" marks, especially on dorsal hands), multiple basal cell carcinomas, and local anhidrosis (decreased or absent sweating).
- Personal and family history of previous nonmelanoma skin cancer (basal cell carcinoma or squamous cell carcinoma): Persons who have been diagnosed with one nonmelanoma skin cancer are at increased risk of developing additional tumors in the future. The risk of developing new nonmelanoma skin cancers is reported to be 35% at 3 years and 50% at 5 years after an initial skin cancer diagnosis.
- Skin type (including albinism)
- Stage 0: Cancer involves only the epidermis and has not spread to the dermis.
- Stage I: Cancer is not large (ie, <2 cm) and has not spread to the lymph nodes or other organs.
- Stage II: The cancer is large (ie, >2 cm) but has not spread to lymph nodes or other organs.
- Stage III: The cancer has spread to tissues beneath the skin (eg, muscle, bone, cartilage), and/or has spread to regional lymph nodes, but has not spread to other organs.
- Stage IV: The cancer can be any size and has spread to other organs.
- Electrodesiccation and curettage: After adequate anesthesia is administered to the patient, the tumor is scraped using a curette, and then the base and lateral margins are electrodesiccated. This is repeated twice.
- Advantages: Electrodesiccation and curettage is a brief procedure (<5 min) and is effective in treating primary nodular and superficial basal cell carcinoma. Cure rates are as high as 95%.
- Disadvantages: The procedure is operator-dependent and often leaves a white atrophic scar. It is less effective on the nose, and the tumor often tracks down pilosebaceous units. This procedure is less effective than Mohs micrographic surgery in treating infiltrating basal cell carcinoma, micronodular basal cell carcinoma, morpheaform (sclerosing) basal cell carcinoma, and recurrent basal cell carcinoma; Mohs micrographic surgery is considered the treatment of choice in most of those cases. The curettage and cauterization procedure is not suitable for patients with cardiac pacemakers or for the treatment of morpheaform lesions, deeply invasive and ulcerated lesions, or recurrent tumors with ill-defined borders.
- Curettage (without desiccation): After adequate anesthesia is administered to the patient, the tumor is scraped using a curette.43 This is often repeated twice more.
- Advantages: This procedure is brief (<5 min) and is effective in treating primary nodular and superficial basal cell carcinoma. Cure rates may be as high as 95%, although it has been studied less than electrodesiccation and curettage. This procedure is believed by some to have a better cosmetic outcome than electrodesiccation and curettage.
- Disadvantages: This procedure is not widely accepted and not commonly performed. The procedure is operator-dependent and often leaves a white atrophic scar. It is less effective on the nose, and the tumor often tracks down pilosebaceous units. This procedure is less effective in treating infiltrating basal cell carcinoma, micronodular basal cell carcinoma, morpheaform (sclerosing) basal cell carcinoma, and recurrent basal cell carcinoma than is Mohs micrographic surgery, which is considered the treatment of choice in most instances.
- Curettage with erbium: YAG laser ablation: After adequate anesthesia is administered to the patient, the tumor is scraped using a curette. The newly formed ulcer is then ablated along with a narrow (<1 mm) margin of adjacent epidermis. This is often repeated 2 more times.
- Advantages: This procedure is brief (<5 min) and is effective in treating primary nodular and superficial basal cell carcinoma. Cure rates may be as high as 95%, although it has been studied less than electrodesiccation and curettage. This procedure is believed by some to have a better cosmetic outcome than electrodesiccation and curettage.
- Disadvantages: This procedure is less commonly performed than electrodesiccation and curettage. The procedure is operator-dependent and may leave a white atrophic scar. It is less effective on the nose, and the tumor often tracks down pilosebaceous units. This procedure is less effective in treating infiltrating basal cell carcinoma, micronodular basal cell carcinoma, morpheaform (sclerosing) basal cell carcinoma, and recurrent basal cell carcinoma than is Mohs micrographic surgery, which is considered the treatment of choice in most instances.
- Surgical excision: After adequate anesthesia is administered to the patient, a No. 15-blade or 10-blade scalpel is used to incise down to the subcutis. To increase the likelihood of complete tumor removal, one must include a margin of normal-appearing skin in order to remove all clinically invisible tumor extension. The larger the amount of clinically normal-appearing skin removed, the higher the cure rate, although the more extensive removal leaves a larger surgical defect and a poorer cosmetic result in most patients. In most circumstances, a 3- to 4-mm margin of normal, clinically uninvolved skin is removed.44 This procedure is normally performed during a skin biopsy procedure.45
- Advantages: Surgical excision usually produces good-to-excellent cosmetic results and cure rates as high as 95%.
- Disadvantages: Surgical excision is operator-dependent, as those more experienced may be better at detecting tumor margins. Excision is less effective in treating tumors without clearly defined clinical margins (eg, infiltrating basal cell carcinoma, micronodular basal cell carcinoma, morpheaform [sclerosing] basal cell carcinoma), and is far less effective in treating recurrent basal cell carcinoma than it is in treating primary basal cell carcinoma.
- Mohs micrographically controlled surgery:46 After adequate anesthesia is administered to the patient, the clinically apparent tumor is often removed by curettage or excision. The surgeon then removes a thin layer of tissue (called stage I), usually less than 1 mm in thickness, of surrounding epidermis and either dermis or subcutis, which then is examined under the microscope. The tumor is removed and processed to allow for localization of any tumor that might persist. This process allows the surgeon to take additional sections (stages) from the location where the tumor persists. According to many authors, this procedure is the criterion standard of care for basal cell carcinoma treatment because it is associated with the lowest recurrence rate.47
- Advantages: Mohs micrographically controlled surgery has the highest cure rate of any treatment modality (99% for primary basal cell carcinoma, 90-95% for recurrent basal cell carcinoma), spares as much uninvolved skin as possible, and is the treatment of choice for infiltrating basal cell carcinoma, micronodular basal cell carcinoma, morpheaform (sclerosing) basal cell carcinoma, and recurrent basal cell carcinoma.
- Disadvantages: Mohs micrographic surgery is time consuming and may be available in only a few centers because it is expensive. Patients might require additional anesthesia before each stage.
- Cryosurgery: Liquid nitrogen is applied to the clinically apparent tumor.48 A temperature probe is inserted into the skin at a lateral margin. Treatment stops when the temperature at the lateral margins reaches -60°C. Most patients suffer pain and swelling after the area thaws. Generally, this procedure is not recommended for basal cell carcinoma, especially for morpheaform lesions, deeply invasive and ulcerated lesions, or recurring tumors with ill-defined borders. Although tissue sparing, this technique temporary leaves the wound open, and scarring or hypopigmentation may result.
- Advantages: Cryosurgery has good cosmetic results and good cure rates when used to treat tumors with well-defined clinical margins (eg, nodular basal cell carcinoma). The procedure is a good option for patients who are not surgical candidates.
- Disadvantages: Cryosurgery is operator-dependent, as accurate clinical detection of tumor margins increases the effectiveness of treatment.
- Plastic surgery: This procedure is very useful for treating lesions larger than 3 mm or for those in a difficult location. Sometimes, surgeons perform this procedure after a simple excision to obtain a more aesthetic result. To perform this procedure, a skin graft or flap is created to repair the defect after excision.49 This technique is especially useful to reduce the amount of scarring or when rapidly closing a wound. Z-plasty is an effective procedure in repairing forehead surgical defects when the size and location of the defect do not otherwise allow for a cosmetically acceptable result.
- Laser surgery:50,51 This procedure uses high-energy rays from a carbon dioxide laser to damage cancer cells and to stop their growth. Routine techniques are not useful in patients with a high risk of bleeding and the indication for laser surgery is limited to superficial basal cell carcinoma. After treatment, some changes in skin may develop, which may become noticeable many years later.
Basal cell carcinoma is also a feature of basal cell nevus syndrome (ie, Gorlin syndrome),15 an autosomal dominant inherited condition. The lesions in these patients cannot be distinguished histologically from ordinary basal cell carcinomas. The gene responsible for this syndrome is located on chromosome arm 9q, and chromosome abnormalities develop in some patients. The number of basal cell carcinomas in patients with this syndrome may number from one to hundreds. Multiple basal cell carcinomas begin to appear after puberty on the face, trunk, and extremities. In many cases, the tumors are highly invasive and involve areas of the face, especially around the eyes and nose.16 Other features associated with Gorlin syndrome (fortunately uncommon) include the following:17
Causes
The exact cause of basal cell carcinoma is unknown. Environmental and genetic factors that are believed to predispose patients to basal cell carcinoma skin cancer include the following:
Laboratory Studies
Since basal cell carcinoma rarely metastasizes, laboratory and imaging studies are rarely clinically indicated in patients presenting with localized lesions.
Procedures
A skin biopsy is often required to confirm the diagnosis and determine the histologic subtype. Most often, a shave biopsy is all that is required. However, in the case of a pigmented lesion where there may be difficulty distinguishing between pigmented basal cell carcinoma and melanoma, an excisional or punch biopsy may be indicated.
Skin biopsy is often curative.
Histologic Findings
Several histologic types of basal cell carcinoma exist, some of which are important because the clinical detection of tumor margins is more difficult with certain histologic types.20 Usually, basal cell carcinomas are well differentiated and cells appear histologically similar to basal cells of epidermis. The characteristic cells of basal cell carcinoma have a large, uniform, oval, nonanaplastic-appearing nucleus with little cytoplasm. The nuclei resemble that of the basal cells of the epidermis, although they have a larger nuclear-to-cytoplasmic ratio and lack intercellular bridges. A mitotic figure is very rarely observed.
A histopathologic examination of paraffin-embedded sections of basal cell carcinoma usually reveals solid cellular strands, collections of cells with dark-staining nuclei and scant cytoplasm.
The peripheral cell mass is in a palisade arrangement that resembles the basal layer of the epidermis, sometimes with pseudocystic aspects, and with a variable number of mitoses.
The connective tissue stroma surrounding the tumor islands is arranged in parallel bundles and often shows young fibroblasts immediately adjacent to the tumor. Each subtype of basal cell carcinoma has a specific histologic pattern (ie, desmoplastic reaction of the morpheaform type, stromal islands separated by basal cells strands of the fibroepithelial type). Artificial retraction of the stroma from the tumor islands is frequently observed histologically. Additionally, the stroma is often mucinous. Cells from recurrent basal cell carcinoma often show squamous aspects.
Histologically, basal cell carcinoma is divided into 2 categories: undifferentiated and differentiated. Basal cell carcinoma with little or no differentiation is referred to as solid basal cell carcinoma and includes pigmented basal cell carcinoma, superficial basal cell carcinoma, sclerosing basal cell carcinoma, and infiltrative basal cell carcinoma (a histologic subtype). Differentiated basal cell carcinoma often has slight differentiation toward cutaneous appendages, including hair (keratotic basal cell carcinoma), sebaceous glands (basal cell carcinoma with sebaceous differentiation), or tubular glands (adenoid basal cell carcinoma). Noduloulcerative (nodular) basal cell carcinoma is usually differentiated.
Histologic types can be summarized as follows:
- Nodular or noduloulcerative basal cell carcinoma, which is the most common type, generally consists of large, round or oval tumor islands within the dermis, often with an epidermal attachment. Artificial retraction of the tumor islands from the surrounding stroma is commonly seen.
- Micronodular basal cell carcinoma is similar to the noduloulcerative type, although the tumor islands are small (often <15 cells in diameter).
- Pigmented basal cell carcinoma consists of large, round or oval tumor islands containing large amounts of melanin within melanocytes and melanophages.
- Cystic basal cell carcinoma consists of large, round or oval tumor islands within the dermis with mucin present within the center of the island.
- Infiltrative basal cell carcinoma is a common type of basal cell carcinoma in which strands of basaloid tumor cells are seen infiltrating between collagen bundles.
- Morpheaform or sclerosing basal cell carcinoma consists of elongated strands of basaloid cells that lead to the adjacent formation of a dense fibrous stroma.
- Superficial basal cell carcinoma consists of buds of basophilic cells within the papillary and occasionally superficial reticular dermis, but they are attached to the epidermis.
DNA mismatch repair (MMR) proteins are a group of proteins that physiologically stimulate G2 cell cycle checkpoint arrest and apoptosis. Failure of MMR proteins to detect induced DNA damage results in the survival of mutating cells. MMR proteins have been recently found to be increased in nonmelanoma skin cancers in comparison with normal skin, and some evidence also exists of MMR dysregulation.21
According to some studies, the so-called fibroepithelioma of Pinkus, considered to be a premalignant skin condition, must be considered as a fenestrated variant of basal cell carcinoma.22,23,24
Staging
Basal cell carcinoma rarely metastasizes and is usually not staged, unless the cancer is very large and is suspected of spreading to other parts of the body. Basal cell carcinoma staging may be similar to the staging of squamous cell carcinoma, which is according to the following scheme:
- Stage 0: Cancer involves only the epidermis and has not spread to the dermis.
- Stage I: Cancer is not large (ie, <2 cm) and has not spread to the lymph nodes or other organs.
- Stage II: The cancer is large (ie, >2 cm) but has not spread to lymph nodes or other organs.
- Stage III: The cancer has spread to tissues beneath the skin (eg, muscle, bone, cartilage), and/or has spread to regional lymph nodes, but has not spread to other organs.
- Stage IV: The cancer can be any size and has spread to other organs.
Medical Care
In nearly all cases, the recommended treatment modality for basal cell carcinoma is surgery.25,26 Some topical treatments exist for some forms of basal cell carcinoma, although generally with cure rates less than that of surgical modalities. Treatments vary according to cancer size, depth, and location. Dermatologists may perform many of the therapies in an outpatient setting. Most therapies are well established and widely applied; nevertheless, researchers still are studying some options (eg, photodynamic therapy with photosensitizers27,28,29 ) and awaiting further reports. Ideally, the treatment options should be evaluated jointly with a surgeon, dermatologist, and radiotherapist and should be based on histologic diagnosis.
- Topical 5-fluorouracil 5% (Efudex): 5-Fluorouracil (5-FU) applied twice daily for 2-12 weeks can be effective in treating superficial basal cell carcinoma, with a reported cure rate as high as 93%.30 The use of 5-fluorouracil for other types of basal cell carcinoma is generally not recommended because it may not penetrate deeply enough into the dermis to eradicate all tumor cells. Irritation and crusting are common and expected; significant irritation and discomfort are not uncommon, but scars are unusual. The recurrence rate is very high.
- Interferon: In a small study by Greenway et al, 1.5 million IU interferon alfa-2b injected intralesionally 3 times per week for 3 weeks resulted in clearing 3 cases of primary nonrecurrent basal cell carcinoma and 5 cases of primary superficial basal cell carcinoma.31 Because larger studies are needed, most practitioners consider this an experimental therapeutic modality. Acetaminophen can be administered to patients who experience the flulike symptoms associated with this therapy.
- Imiquimod: Imiquimod cream (Aldara) is FDA approved for the treatment of superficial32 basal cell carcinoma excluding the face. Several studies have shown imiquimod to be curative in all patients with superficial basal cell carcinoma if used twice a day, and in 73-82% of patients when used once a day for 6-12 weeks. Smaller studies have shown similar responses for nodular basal cell carcinoma. Studies for other histologic types of basal cell carcinoma are currently underway. Treatment is usually initiated at 3 times per week and increased as tolerated to once daily, and even twice daily if tolerated, to maintain mild-to-moderate skin irritation.33,34 Patients can titrate the frequency of application to maintain low-to-moderate skin irritation. A 12-week course of treatment is often used, which does not need be contiguous.35
- GDC-0449: At the 2008 meeting of the American Association for Cancer Research, a preliminary report was presented on very promising results in locally advanced, multifocal, and metastatic basal cell carcinoma with a novel new compound labeled for now as GDC-0449. This compound is a synthetic chemical designed to reproduce the properties of cyclopamine, a naturally occurring compound. GDC-0449 blocks the Hedgehog pathway in cells. This pathway contains 2 genes, PTCH and SMO, which lead to a known tumor promoting gene, GLI1. A change in any of these genes has been associated with the development of basal cell carcinoma.
- GDC-0449 is given orally once a day. Its side effects are relatively minor: some loss of sense of taste and some loss of hair and loss of weight. In the first clinical trial of GDC-0449, eight ninths of the patients responded to treatment with tumor shrinkage or stabilization. Decreased amounts of GLI1 were found in the skin of patients after treatment.
- Subjects in this trial have experienced lasting clinical benefit, and follow-up studies in a wider range of patients and larger groups of patients will be eagerly awaited.36,37
- Radiotherapy (RT): Basal cell carcinomas are usually radiosensitive, and RT can be used for advanced and extended lesions and in patients for whom surgery is not suitable (eg, because of allergy to anesthetics, current anticoagulant therapy, a tendency to form keloids,38 or facial tumors). RT may also be used as adjuvant therapy in high-risk malignancies. Although RT was used extensively in the past because of its high cure rate (95%), it is now used sparingly because it is time consuming and expensive.
- RT is contraindicated in young patients, because of the high risk of radiodermatitis and scars; in lesions on the trunk and extremities; and in delayed cancer recurrence (eg, especially in patients previously treated with radiation). RT is also contraindicated in patients with connective tissue diseases or genetic conditions predisposing to skin cancer (eg, xeroderma pigmentosum). RT requires multiple visits. Treatment results in radiation damage and, therefore, should be reserved for older patients. RT is less effective for nonfacial tumors.
- Ionizing radiation: Superficial x-ray treatment is usually administered in 10 sessions of 4 gray (Gy) (400 rad). Electrons (electron beam) can be used and many radiation oncologists prefer this treatment method over superficial x-rays.
- Photodynamic therapy (PDT): A photosensitizing drug (ie, porphyrin, 5-ALA) is administered orally or parenterally, as well as applied topically, and localizes into tumor cells before activation by exposure to light (eg, laser). The efficacy is low, and this treatment is frequently used as palliation. Photodynamic therapy may cause local edema, erythema, blistering, and ulceration, but the final cosmetic effect is good.
- Systemic retinoids: Many reports show some efficacy for currently available systemic retinoids, but the long-term toxicity of these agents limits their application for most patients.39
Further information about basal cell carcinoma therapy is available from the National Comprehensive Cancer Network (NCCN) at Basal Cell and Squamous Cell Skin Cancers and at Guidelines for the Management of Basal Cell Carcinoma.
Surgical Care
The goal of therapy for patients with basal cell carcinoma is removal of the tumor with the best possible cosmetic result. By far, surgical modalities are the most studied, most effective, and most used treatments for basal cell carcinoma. The effectiveness of surgical modalities depends heavily on the surgeon's skills; considerable differences in cure rates have been observed among surgeons. Modalities used include electrodesiccation and curettage, excisional surgery, Mohs micrographically controlled surgery, and cryosurgery.35,40,41
Selection of the modality depends on whether the tumor is primary or recurrent, as well as on its location, size, and histologic type. The American Academy of Dermatology has published guidelines regarding the treatment of basal cell carcinoma.42
Knowledge of the behavior of the different clinical and pathologic types of basal cell carcinoma is essential in choosing the appropriate therapy. The traditional surgical options involve the use of simple excision, cryosurgery, electrodesiccation, and curettage. Basal cell carcinoma recurrence after irradiation makes surgery mandatory.
|
|
|
|