JELLYFISH
Sea Nettles.
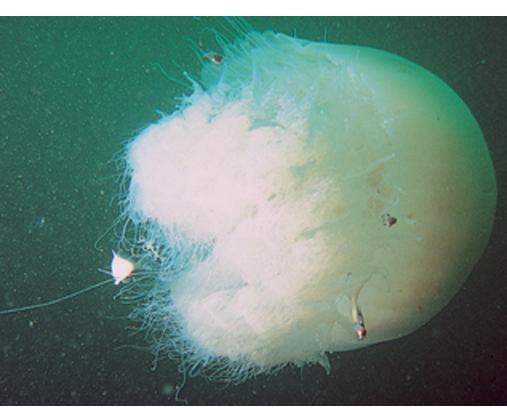
Among the organisms most commonly causing jellyfish stings are the sea nettles, which comprise two different species, both of which inhabit Atlantic as well as Indo-Pacific waters. Cyanea capillata and its relatives is the larger of the two species, with a bell measuring up to 1 m and numerous tentacles reaching 30 m in length. Chrysaora quinquecirrha is smaller, with a white or rusty bell that may reach 30 cm with four digestive tentacles hanging from it. Although sea nettle stings are seldom lethal, they can be quite painful. Initially the victim experiences a sharp burning pain in the area contacted by the tentacles. Within minutes, the sting area develops a zigzag, whip-like pattern of raised red welts 2 to 3 mm wide .The duration of acute pain may vary, but the pain often begins to abate in 30 minutes. The wheals usually subside by 1 hour, but purplish brown petechial and post-inflammatory pigmentation may persist for several days.
Portuguese Man-of-War.
Physalia physalis is the species name for the Portuguese man-of-war, which is a member of the class Hydrozoa and is therefore not a true jellyfish. P. physalis is encountered in both Atlantic and Mediterranean waters, and is easily recognized by its translucent blue to pink or purple bladder-like float with multiple tentacles . P. physalis is distinguished from its Pacific ocean relative P. utriculus, commonly known as the blue bottle, by its larger bell, which ranges in size from 10 to 30 cm, and multiple fishing tentacles extending up to 30 m; in contrast, P. utriculus has only a single tentacle that rarely exceeds 5 m. These tentacles are armed along their entire length with hundreds of thousands of nematocysts arranged in stinging batteries, with each battery containing hundreds of nematocysts. The nematocysts remain active even after portions of the tentacles are broken off in storms or when these animals are stranded on the shoreline by high winds or waves. A beached Portuguese man-of-war can cause a severe sting when stepped on or touched. Children who are stung after handling these animals and then cry and rub their eyes may develop an acute conjunctivitis.
Stings of P. physalis are more painful and severe than those caused by sea nettles and are more extensive and serious than those caused by P. utriculus. At the moment of contact with the tentacles of P. physalis, the victim experiences a sharp, shock-like, burning pain. There may be painful paresthesias or numbness in the sting area. Initially, the sting area appears as an irregular single line or multiple lines composed of red papules, beaded streaks, or erythematous welts that correspond to the areas of tentacle contact. The wheals resolve in hours but may progress to vesicular, hemorrhagic, necrotic, or ulcerative stages before healing .
Post-inflammatory striae may persist for weeks to months. Severe localized complications of P. physalis stings may also include arterial spasm in the sting site that can result in distal digital gangrene.
Within 10 to 15 minutes of a Physalia sting, the victim may develop symptoms of an envenomation reaction characterized by nausea, abdominal cramps, muscular pains, backache, irritability, dyspnea, and chest tightness. Intravascular hemolysis and acute renal failure were reported in a 4-year-old girl after a severe sting by P. physalis. Most reports of death due to stings of P. physalis are not well documented, but well-substantiated case reports of human fatalities do exist.
Cubomedusae [Class Cubozoa]: Box Jellyfish.
Of all the species of jellyfish that cause painful stings and distress to swimmers, the species with the most established record of lethality are the cubozoans. Chironex fleckeri or box jellyfish causes at least one death each year in Australia. The fatality is usually a child, presumably because the size of the victim and the total area of the sting determine the likelihood of death. Until recently, most of the published cases of C. fleckeri stings involved fatal or nearly fatal envenomations, but less serious stings do occur in endemic areas.
C. fleckeri (commonly known as the sea wasp) is an advanced species of jellyfish, with a semitransparent cubic bell that may grow to a volume of 9 L and weigh more than 6 kg . Trailing from the bell are up to 60 stinging tentacles, which may reach 2 to 3 m in length. When a human comes into contact with a box jellyfish, some of the tentacles are torn off and adhere to the skin. Rescuers of C. fleckeri sting victims must exercise caution, because they also are at risk of envenomation until the tentacles have been neutralized and removed.
The stings appear initially as linear welts that give the patient the appearance of having been whipped.45 Fresh stings of C. fleckeri are easily recognized
because they have a diagnostic, frosted, cross-hatched or ladder-like appearance . Microscopic diagnosis is also possible from blade scrapings or tape strippings from the sting site. The intense pain may persist for many hours. Severely stung areas of skin take on a dusky cyanotic appearance and blister formation and necrosis may occur. The healing process is slow and may be complicated by bacterial superinfection and scarring.
Death may ensue within minutes due to cardiotoxic and neurotoxic agents in the venom that can produce ventricular arrhythmias and cardiac arrest, and respiratory failure, respectively. Intravascular hemolysis caused by the toxin can precipitate acute renal failure. First aid for these victims frequently involves cardiopulmonary resuscitation. Intravenous verapamil has been proposed for both treatment and prophylaxis of ventricular arrhythmias. Antivenin is available for C. fleckeri stings, and its early use in severe envenomations may be lifesaving and significantly reduces the pain and inflammation at the sting site.
Irukandji syndrome is a severe and delayed response (usually 30 minutes but between 5 and 40 minutes) to the sting of a small box jellyfish, termed the Irukandji jellyfish, that has resulted in the death of two tourists in the Cairns-Port Douglas region of Australia. The classic syndrome consists of local signs of inflammation together with severe back pain, excruciating muscle cramps, piloerection, sweating, nausea, vomiting, headache, and palpitations. The most severe cases may progress to include extreme hypertension and cardiac failure. Only one species, Carukia barnesi, has been clearly linked to this syndrome, but it is thought that at least six different species of small jellyfish, each with only one tentacle arising from each corner of the bell (carybdeids), may be etiologic agents. The stings most often occur in deep water. Treatment includes application of vinegar to discharge nematocysts and victim transport for medical attention including pain control and α blockade, because the venom is thought to act as a presynaptic neuronal sodium agonist and to stimulate norepinephrine release.
Prevention and Treatment of Jellyfish Stings.
Tables 209-2, 209-3, and 209-4 give details on the prevention of jellyfish stings and first aid for and treatment of the stings. Systemic reactions may occur, and the treatment for these includes support of vital functions with cardiopulmonary resuscitation, oxygen, and intravenous fluids. Application of a venous-lymphatic constriction bandage proximal to the wound site should be considered in the case of severe stings when systemic reactions are present or likely to occur, when topical deactivation of tentacles is not possible, and when transport to receive specific antivenin for C. fleckeri stings is available. The antivenin is prepared from sheep serum and may therefore pose a risk of allergic reaction in sensitive individuals. The preferred route of administration is intravenous, but the antivenin may be given intramuscularly. In severe stingings, it has proved lifesaving. It is also the only treatment that can alleviate the intense pain and may reduce inflammation at the
sting site and decrease the chance of scarring. Intravenous administration of verapamil has been advocated for both treatment and prophylaxis of arrhythmias. For pain in severe stingings, parenteral narcotic analgesics and ice packs, as well as antivenin, should be considered. Local reactions may be treated with topical anesthetic ointments, creams, lotions, or sprays to relieve itching or burning pain. For delayed-type hypersensitivity reactions, topical glucocorticoids, antihistamines, and systemic glucocorticoids should be used if necessary.
|
TABLE 209-2 Prevention of Jellyfish Stings
|
|
1. Swim only at patrolled beaches with properly trained lifeguards and adequate treatment facilities.
2. Avoid swimming in infested waters, especially after a storm, because stings may result from remnants of floating damaged tentacles.
3. Beware of apparently dead or beached jellyfish.
4. When snorkeling or scuba diving, wear protective clothing such as a wet suit, long-sleeved shirt, pants or long woolen underwear, and gloves. In areas where Irukandji syndrome occurs, wear a Lycra stinger suit.
5. Use sunblock containing jellyfish and “sea lice” repellent.
6. Bathing beaches should be closed during periods of high jellyfish infestation.
|
|
Data from McKinney PE: Out-of-hospital and inter-hospital management of crotaline snakebite. Ann Emerg Med 37:168, 2001; Kimball AB et al: Efficacy of a jellyfish sting inhibitor in preventing jellyfish stings in normal volunteers. Wilderness Environ Med 15:102, 2004; and Harrison SL et al: Reported knowledge, perceptions, and behavior of tourists and North Queensland residents at risk of contact with jellyfish that cause the “Irukandji syndrome.” Wilderness Environ Med 15:4, 2004.
|
|
|
TABLE 209-3 First Aid Treatment of Jellyfish Stings
|
|
1. Remove or rescue the victim from the water.
2. Stabilize vital functions: Airway, breathing, circulation.
3. Immobilize the affected part to prevent further envenomation by adherent tentacles.
4. Identify the type of jellyfish sting by considering locale, time of year, and indigenous species and by observing the sting pattern. Preserve a portion of the tentacle for future identification. Tape-strip or scrape the sting site for microscopic analysis of the nematocysts if no tentacles are available.
5. To prevent further envenomation of the victim and to reduce the chance of a sting to the rescuer, disarm the nematocysts before removing the adherent tentacles.
|
|
Data from refs. 46, 47, 52, 53, 105, and 106.
|
|
|
TABLE 209-4 Organism-Specific and Follow-Up Treatment of Jellyfish Stings
|
|
1. If Chironex fleckeri or other box jellyfish species that cause the Irukandji syndrome are suspected, douse or spray dilute acetic acid (3%-10%) or household vinegar over all areas of tentacle contact for at least 30 s.
2. For sea nettles, mix sodium bicarbonate (baking soda) with water to form a slurry and pour over the affected area or apply the powder directly to the tentacles.107
3. For Physalia physalis stings, a slurry of baking soda is indicated. Vinegar had been reported to neutralize nematocysts of P. physalis, but work with species from Australia indicate that it may cause a discharge of nematocysts in some cases.
4. If vinegar or baking soda is unavailable, papain, available as a powdered meat tenderizer, may be applied directly as a powder or mixed in water as a slurry to sting areas and tentacles of both sea nettles and Portuguese man-of-war.
5. If nothing else is available, the tentacles can be rinsed off with seawater.
6. Do not use fresh water, methylated spirits, or alcohol in any form to deactivate tentacles, because these all may cause a rapid massive discharge of nematocysts.
7. After the tentacles have been disarmed, they may be carefully removed with a forceps or gently scraped away from the skin with shaving cream and a razor or a plastic card, shell, or knife.
|
|
Secondary infections should be treated with the appropriate parenteral antibiotics, and antitetanus therapy should be considered. Application of ice or cold packs can relieve the pain of mild to moderate stings of many types of jellyfish, and aspirin or acetaminophen, alone or in combination with codeine, can be used to relieve persistent pain.