|
Xeroderma Pigmentosum
XP serves as the prototype heritable disease with increased sensitivity to cellular injury. XP is an autosomal recessive disease with sun sensitivity, photophobia, early onset of freckling, and subsequent neoplastic changes on sun-exposed surfaces. There is cellular hypersensitivity to UV radiation and to certain chemicals in association with abnormal DNA repair. Some of the patients have progressive neurologic degeneration.
FREQUENCY
XP occurs with an estimated frequency of 1 in 1 million persons in the United States and 1 per 100,000 thousand people in Japan.15 It is relatively more common in areas such as the Middle East where marriage of close relatives is practiced. Patients have been reported worldwide in all races, including whites, Asians, blacks, and Native Americans.
CLINICAL FEATURES
Skin.
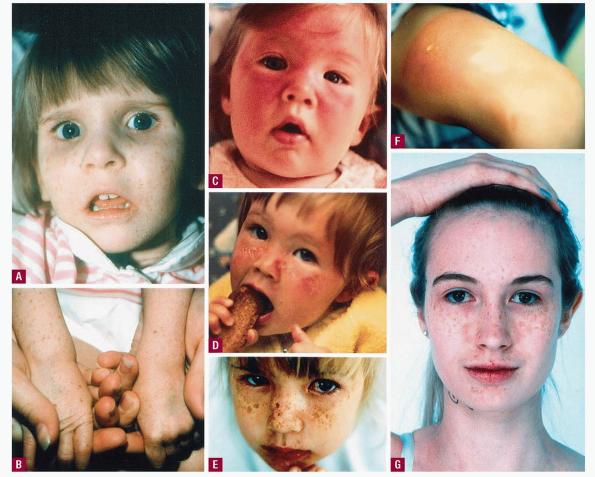
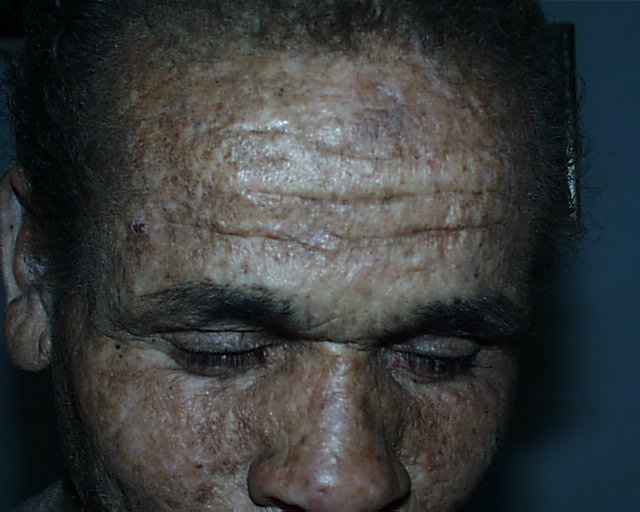
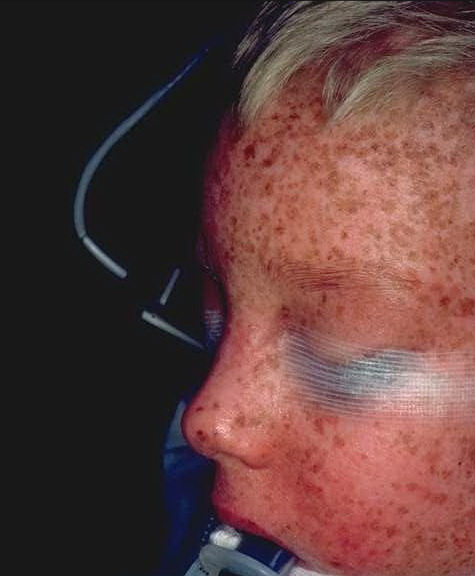
Approximately one-half the patients with XP have a history of acute sunburn reaction on minimal UV exposure. The other patients tan normally without excessive burning. In all patients, numerous freckle-like hyperpigmented macules appear predominately on sun-exposed skin . The median age of onset of the cutaneous symptoms in XP is between 1 and 2 years . These generally spare sun-protected sites such as the buttocks . However, some severely sun-exposed patients may show pigmentary abnormalities in the axillae. Continued sun exposure causes the patient's skin to become dry and parchment-like, with increased pigmentation, hence the name xeroderma pigmentosum . Pre-malignant actinic keratoses develop at an early age . The appearance of sun-exposed skin in children with XP is similar to that occurring in farmers and sailors after many years of extreme sun exposure.
Cancer.
Patients with XP younger than 20 years of age have a greater than 1000-fold increased risk of cutaneous basal cell carcinoma, squamous cell carcinoma, or melanoma. The median age of onset of non-melanoma skin cancer reported in patients with XP is 8 years. This 50-year reduction in comparison with the general population is an indication of the importance of DNA repair in protection from skin cancer in unaffected individuals . Multiple primary cutaneous neoplasms, including melanomas, occur commonly in XP patients.
Review of the world's literature on XP has revealed a substantial number of cases of oral cavity neoplasms, particularly squamous cell carcinoma of the tip of the tongue, a presumed sun-exposed location. Brain (sarcoma and medullo-blastoma), central nervous system (astrocytoma of the spinal cord), lung, uterine, breast, pancreatic, gastric, renal, and testicular tumors and leukemia have been reported in a few patients with XP. Overall, these reports suggest an approximate 10- to 20-fold increase in internal neoplasms in XP.
Eyes.
Ocular abnormalities are almost as common as the cutaneous abnormalities and are an important feature of XP . The posterior portion of the eye (retina) is shielded from UV radiation by the anterior portion (lids, cornea, and conjunctiva). Clinical findings are strikingly limited to these anterior, UV-exposed structures. Photophobia is often
present and may be associated with prominent conjunctival injection. Schirmer's testing frequently reveals reduced tearing leading to dry eyes. Continued UV exposure of the eye may result in severe keratitis, leading to corneal opacification and vascularization. The lids develop increased pigmentation and loss of lashes. Atrophy of the skin of the lids results in ectropion, entropion, or, in severe cases, complete loss of the lids. Benign conjunctival inflammatory masses or papillomas of the lids may be present. Epithelioma, squamous cell carcinoma, and melanoma of UV-exposed portions of the eye are common. The ocular manifestations may be more severe in black patients.
Neurologic System.
Neurologic abnormalities have been reported in approximately 30 percent of the patients. The onset may be early in infancy or, in some patients, delayed until the second decade. The neurologic abnormalities may be mild (e.g., isolated hyporeflexia) or severe, with progressive mental retardation, sensorineural deafness (beginning with high-frequency hearing loss), spasticity, or seizures. The most severe form, known as the De Sanctis-Cacchione syndrome, involves the cutaneous and ocular manifestations of classic XP plus additional neurologic and somatic abnormalities, including microcephaly, progressive mental deterioration, low intelligence, hyporeflexia or areflexia, choreoathetosis, ataxia, spasticity, Achilles tendon shortening leading to eventual quadriparesis, dwarfism, and immature sexual development. The complete De Sanctis-Cacchione syndrome has been recognized in very few patients; however, many patients with XP have one or more of its neurologic features. In clinical practice, deep tendon reflex testing and routine audiometry usually can serve as a screen for the presence of XP-associated neurologic abnormalities. In cases where there is clinical evidence of early neurologic abnormalities, a brain magnetic resonance imaging (MRI) may show enlarged ventricles.
The predominant neuropathologic abnormality found at autopsy in patients with neurologic symptoms was loss (or absence) of neurons, particularly in the cerebrum and cerebellum. There is evidence for a primary axonal degeneration in these patients.19
LABORATORY ABNORMALITIES
Cellular Hypersensitivity.
Cultured cells from patients with XP generally grow normally when not exposed to damaging agents. The population growth rate or single-cell colony-forming ability is reduced to a greater extent than normal, however, after exposure to UV radiation. A range of post-UV colony-forming abilities has been found with fibroblasts from patients, some having extremely low post-UV colony-forming ability and others having nearly normal survival .
XP fibroblasts are deficient in their ability to repair some UV-damaged viruses or plasmids to a functionally active state. These host cell reactivation assays have detected an abnormality in every form of XP tested.
UV-irradiated XP fibroblasts are hypermutable compared to normal fibroblasts. This post-UV hypermutability is believed to be the basis of the increased frequency of sunlight-induced somatic mutations that lead to cancer in XP patients.21
Chromosome Abnormalities.
XP cells generally are found to have a normal karyotype without excessive chromosome breakage or increased sister chromatid exchanges (as seen in Bloom syndrome). After exposure to UV radiation, however, abnormally large increases in chromosome breakage and in sister chromatid exchanges have been observed. The extent of this induced abnormality varies in different patients.
DNA Repair.
In 1968, hypersensitivity of cultured XP cells to UV damage was reported by Cleaverto be the result of defective DNA repair. He found defective UV-induced repair replication, indicating a defect in the NER pathway. Most XP cells have a normal response to treatment with x-rays, indicating the specificity of the DNA repair defect. The defective genes for the seven NER-defective forms of XP and the XP variant have been cloned24 and their functions are being investigated (see Chap. 109).
Complementation Groups.
Genetic heterogeneity among the XP DNA repair defects was found by fusing cultured fibroblasts from different patients and defining complementation groups (see Chap. 109). Up to 2006, seven such DNA excision repair-deficient complementation groups have been identified (named XP-A to XP-G) and the corresponding genes have been identified . Additional patients with clinical XP but normal NER have been called XP variants. Studies of cellular hypersensitivity revealed a slightly increased sensitivity to UV-induced inhibition of cell growth that was potentiated by caffeine. Cells from XP-variant patients have a defect in an error-prone DNA polymerase (pol eta) that bypasses unrepaired DNA damage.
Prenatal Diagnosis.
Prenatal diagnosis has been reported by measuring UV-induced unscheduled DNA synthesis in cultured amniotic fluid cells and by use of DNA diagnosis of trophoblast cells obtained early in pregnancy.
Drug and Chemical Hypersensitivity.
A number of DNA-damaging agents other than UV radiation have been found to yield hypersensitive responses with XP cells. These agents include drugs (psoralens, chlorpromazine), cancer chemotherapeutic agents (cisplatin, carmustine), and chemical carcinogens (benzo[a]pyrene derivatives). Presumably, these agents induce DNA damage whose repair involves portions of the DNA repair pathways that are defective in XP.
TREATMENT
Management of patients with XP is based on early diagnosis, lifelong protection from UV radiation exposure, and early detection and treatment of neoplasms. Diagnosis rests on recognition of the characteristic clinical features and is confirmed by laboratory tests of cellular hypersensitivity to UV and defective DNA repair (see Chap. 109). Molecular determination of disease-causing mutations may soon move from only being performed in research laboratories to being certified for clinical testing.
Sun Protection.
Patients should be educated to protect all body surfaces from UV radiation by wearing protective clothing and UV-absorbing glasses and long hair styles. They should adopt a lifestyle to minimize UV exposure and use sunscreens with high sun protective factor (SPF) ratings (minimum SPF 15) daily. Patients should be examined frequently by a family member who has been instructed in recognition of cutaneous neoplasms. A set of color photographs of the entire skin surface with close-ups of lesions (including a ruler) is often extremely useful to both the patient and the physician in detecting new lesions. A physician should examine patients at frequent intervals (approximately every 3 to 6 months depending on severity of skin disease). Pre-malignant lesions such as actinic keratoses may be treated by freezing with liquid nitrogen, or with topical 5-fluorouracil or imiquimod. Photodynamic therapy, using, for example,
the topical photosensitizer 5-aminolevulinic acid followed by exposure to blue light, is an effective treatment modality for normal patients with multiple actinic keratoses. There are no data on the safety or efficacy of this treatment in XP patients. Caution is recommended because an abnormal response to photodynamic therapy or other light- or laser-based therapies cannot be excluded in XP cells. Larger areas have been treated with therapeutic dermatome shaving or dermabrasion to remove the more damaged superficial epidermal layers. This procedure permits repopulation by relatively UV-shielded cells from the follicles and glands.
Because cells from patients with XP are also hypersensitive to environmental mutagens such as benzo[a]pyrene found in cigarette smoke, prudence dictates that patients should be protected against these agents. One of our patients who smoked cigarettes for more than 10 years died of bronchogenic carcinoma of the lungs at age 35 years and another patient who smoked has developed a lung cancer at age 48 years.34 Thus, we recommend that XP patients refrain from smoking cigarettes and that parents should protect children with XP from being exposed to second-hand smoke.
Cancers.
Cutaneous neoplasms are treated in the same manner as in patients who do not have XP. This involves electrodesiccation and curettage, surgical excision, or Mohs micrographic surgery . Because multiple surgical procedures are often necessary, removal of undamaged skin should be minimized. Extremely severe cases have been treated by excision of large portions of the facial surface and grafting with uninvolved skin.
Most patients with XP are not abnormally sensitive to therapeutic x-rays, and XP patients have responded normally to full doses of therapeutic x-radiation for treatment of inoperable neoplasms such as an astrocytoma of the spinal cord,17 a frontal lobe astrocytoma, or recurrent squamous cell carcinoma in the orbit. However, cultured cells from two XP patients were found to be hypersensitive to x-rays, so when x-ray therapy is indicated, an initial small dose is advisable to test for clinical hypersensitivity.
Oral isotretinoin has been shown in a controlled study to be effective in preventing new neoplasms in patients with multiple skin cancers.37 Because of its toxicity (hepatic, hyperlipidemic, teratogenic, calcification of ligaments and tendons, premature closure of the epiphyses), oral isotretinoin should be reserved for patients with XP who are actively developing large numbers of new skin cancers. We found that the effective dose varies among patients and some patients may respond to doses of oral isotretinoin as low as 0.5 mg/kg/day.
A bacterial DNA repair enzyme, den V T4 endonuclease, in a topical liposome-containing preparation, has been reported to reduce the frequency of new actinic keratoses and basal cell carcinomas in XP patients in one research study.38 As of 2007, this treatment has not yet been approved by the U.S. Food and Drug Administration.
A study treating multiple melanoma in situ lesions with intralesional interferon-α in one XP patient showed localized clearing only of lesions injected with the intralesional interferon-α but not with the control diluent.39 There are several case reports of XP patients responding to topical treatment with the immune modulator imiquimod . However, none of these reports long-term follow-up.
Eyes.
The eyes should be protected by wearing UV-absorbing glasses with side shields. Methyl cellulose eyedrops can be used to keep the cornea moist. Corneal transplantation has restored vision in patients with corneal opacity from severe keratitis. However, some of these suffered graft rejection due to neovascularization. Neoplasms of the lids, conjunctiva, and cornea are usually treated surgically. We are examining the possibility of using a swab to obtain cytologic specimens from the surface of the eye to determine if early neoplasms can be detected or excluded without the need for performing biopsies.
CLINICAL-LABORATORY CORRELATIONS
Patients with XP are hypersensitive to UV radiation, as are their cultured cells. Cutaneous and ocular abnormalities are strikingly limited to UV-exposed areas and usually spare such UV-shielded locations as the axillae, buttocks, and retina. The fact that black patients with XP have an increased frequency of skin cancer indicates that a normally functioning DNA repair system provides greater protection against skin cancer than does the natural pigmentation of black skin.
Complementation Groups.
At least eight different molecular defects are associated with the clinical abnormalities recognized as XP, as indicated by the existence of seven DNA excision repair-deficient complementation groups (A to G) and the variant form. A discussion of the cloned XP genes and their function can be found in Chapter 109. There is a complex relationship among the DNA repair genes and clinical disease (see Fig. 140-1). Eleven NER genes are associated with at least seven different clinical phenotypes. A clinical phenotype can be associated with defects in each of several genes. Conversely, mutations in one gene can be associated with several different clinical phenotypes. These complex relationships and the roles of DNA repair genes in regulation of transcription and in immune functions are under intense investigation.
COMPLEMENTATION GROUP A.
Complementation group A contains patients with the most severe neurologic and somatic abnormalities (the De Sanctis-Cacchione syndrome) as well as patients with minimal or no neurologic abnormalities.12 Long-term follow-up of these patients has revealed a relationship between the genotype and the phenotype. Patients with the most severe disease appear to have truncating mutations in both alleles of the XPA gene leading to no detectible normal protein. In contrast, patients with minimal neurologic abnormalities have splice-site mutations that permit a small amount of normal messenger RNA (mRNA) to be made. This form is seen in the United States, Europe, and the Middle East. It is the most common form of XP in Japan. Approximately 90 percent of Japanese XP-A patients have the same single-base-substitution founder mutation.47 This finding has served as the basis for development of a rapid diagnostic assay for Japanese XP-A patients (including prenatal diagnosis) using polymerase chain reaction analysis of a small sample of DNA.33 Heterozygous carriers of this disease-causing mutation who have one mutated allele and one normal allele have been estimated to comprise approximately 1 percent of the Japanese population.
COMPLEMENTATION GROUP B.
Complementation group B is composed of five patients in four kindreds who had the cutaneous abnormalities characteristic of XP (including neoplasms) in conjunction with neurologic and ocular abnormalities typical of CS. Another family had two adult sisters with XP without CS who had ocular melanomas and were parents of normal children. Surprisingly, a patient with TTD also was found to have a defect in the XPB gene.
COMPLEMENTATION GROUP C.
Patients in complementation group C , with rare exceptions, have XP with skin and ocular involvement but without neurologic abnormalities. This is the most common group in the United States, Europe, and Egypt, but has been found rarely in Japan. Most patients have truncating mutations in both alleles leading to undetectable levels of XPC mRNA (due to nonsense-mediated message decay). However, a splice lariat branchpoint mutation resulting in as little as 3 percent to 5 percent of normal mRNA resulted in milder clinical symptoms in one family in Turkey. XP-C patients typically do not give a history of severe burning on minimal sun exposure and at times are first diagnosed with the appearance of skin cancer in a child. One XP-C patient was reported to be hypersensitive to ionizing radiation; however, correction of the XPC gene defect did not correct the cellular ionizing radiation hypersensitivity, suggesting that more than one gene was defective in this patient.
COMPLEMENTATION GROUP D.
Patients in complementation group D have been described with six different clinical phenotypes . They may have cutaneous XP with late onset of neurologic abnormalities in their second decade of life or XP with no neurologic abnormalities. Two XP-D patients have been reported with clinical symptoms of both XP and CS. Cells from patients with a photosensitive form of TTD (without XP) also were assigned to the XP complementation group D. Two patients were reported with combined symptoms of both TTD and XP (one patient had a skin cancer) and mutations in the XPD gene. Finally, a patient with cerebro-oculo-facio-skeletal (COFS) syndrome had a mutation in the XPD gene.
COMPLEMENTATION GROUP E.
Complementation group E was found in one kindred in Europe and several in Japan . These patients had relatively mild cutaneous abnormalities without neurologic involvement.
COMPLEMENTATION GROUP F.
Complementation group F patients have been found mainly in Japan. Most of these patients have mild clinical symptoms without neurologic abnormalities or skin cancer. However, we recently found two families with adult onset of severe neurodegeneration with mutations in the XPF gene. The residual rate of DNA repair, however, is very low (only 10 percent to 20 percent of normal).
COMPLEMENTATION GROUP G.
Thirteen patients in XP complementation group G have been identified in the United States, Europe, and Japan . There is a large variation in clinical features among these patients. Several patients with mutations in the XPG gene had clinical features of both XP and severe CS with cachexia and death in the first decade . Other patients with different mutations in the same gene had no neurologic abnormalities.
XERODERMA PIGMENTOSUM VARIANT.
XP-variant cells have normal DNA NER and thus do not fall into any of the complementation groups of cells with defective DNA excision repair . There is, however, a defect in an error-prone, translesional DNA damage bypass polymerase, pol eta . Most XP-variant patients have clinical XP with no neurologic abnormalities. The cutaneous and ocular abnormalities have been severe in some patients and mild in others.
Heterozygotes.
XP heterozygotes (parents and some other relatives) are carriers of the gene for XP but are clinically normal. There is limited epidemiologic evidence to indicate that such persons have an increased risk of developing skin cancer.7 Most tests of cell function or DNA repair yield normal responses with cells from XP heterozygotes.
|

