| Breast cancer= سرطان الثدي |
|
|
Breast cancer
Worldwide, breast cancer is the most frequently diagnosed life-threatening cancer in women and the leading cause of cancer death among women. Over the last two decades, breast cancer research has lead to extraordinary progress in our understanding of the disease, resulting in more efficient and less toxic treatments. Increased public awareness and improved screening have led to earlier diagnosis at stages amenable to complete surgical resection and curative therapies. Consequently, survival rates for breast cancer have improved significantly, particularly in younger women. This article addresses the etiology, clinical presentation, diagnosis, surgical and medical treatment, and prognosis of breast cancer. For patient education resources, visit eMedicine's Cancer and Tumors Center, Women's Health Center, and Imaging Center. eMedicine also has pertinent patient education articles on Breast Cancer, Mastectomy, Breast Lumps and Pain, Breast Self-Exam, Mammogram, and OvarianCancer. EpidemiologyThe American Cancer Society estimated nearly 1.4 million new cases of invasive breast cancer worldwide in 2008. Female breast cancer incidence rates for 2002 varied internationally by more than 2.5-fold, ranging from 3.9 cases per 100,000 in Mozambique to 101.1 cases per 100,000 in the United States. Over the past 25 years, breast cancer incidence rates have risen globally, with the highest rates occurring in the westernized countries. Reasons for this trend include change in reproductive patterns, increased screening, dietary changes, and decreased activity. Although breast cancer incidence is on the rise globally, breast cancer mortality has been decreasing, especially in industrialized countries. In the United States, an estimated 192,370 new cases of invasive breast cancer will occur in women in 2009, along with 1,910 cases in men. After two decades of increasing incidence rates, the number of new female breast cancers decreased by 2.2% per year from 1999 to 2005. This decrease is thought to reflect reduced use of hormone replacement therapy (HRT) following the publication of the Women’s Health Initiative in 2002, which linked HRT use to an increased risk of heart disease and breast cancer. In addition to invasive breast cancer, 62,280 new cases of in situ breast cancer are expected to occur among women in 2009. Approximately 85% of these are expected to be ductal carcinoma in situ (DCIS). Rates of DCIS have stabilized since 2000.1 The current lifetime risk of breast cancer in the United States is estimated at 12.7% for all women, 13.3% for non-Hispanic whites, and 9.98% for African American women. Overall, the annual incidence rates in African American women (119.4 out of every 100,000) and Hispanic/Latina women (89.9 out of every 100,000) have been stable since the early 1990s and are lower than the annual incidence of breast cancer in white women (141.1 out of every 100,000). However, African American women are more likely than white women to be diagnosed with larger, advanced stage tumors (>5 cm). Incidence rates among Asian and Pacific Islander women have continued to increase at 1.5% per year (89 out of every 100,000) but are still significantly lower than white women. Death rates from breast cancer have steadily decreased in women since 1990. An estimated 40,610 breast cancer deaths (40,170 women, 440 men) are expected in 2009. The largest decrease in mortality has been seen in women younger than 50 years (3.3% per year) versus those aged 50 years and older (2.0% per year). The decrease in breast cancer death rates is thought to represent progress in both earlier detection and improved treatment modalities.2 EtiologyThe current understanding of breast tumorigenesis is that invasive cancers arise through a series of molecular alterations at the cellular level, resulting in the outgrowth and spread of breast epithelial cells with immortal features and uncontrolled growth. Genomic profiling has demonstrated the presence of discrete breast tumor subtypes with distinct clinical behavior (eg, 4 subclasses: luminal A, luminal B, basal, and HER2+). The exact number of disease subtypes and molecular alterations from which these subtypes derive remains to be fully elucidated, but they generally align closely with the presence or absence of hormone receptor and mammary epithelial cell type (luminal or basal). The figure below summarizes the current general understanding of breast tumor subtypes, prevalence, and the major associated molecular alterations. This view of breast cancer, not as a set of stochastic molecular events, but as a limited set of separable diseases of distinct molecular and cellular origins, has altered thinking about breast cancer etiology, type-specific risk factors, prevention, and treatment strategies Risk factors Epidemiological studies have identified many risk factors, which increase the chance of a woman developing breast cancer (see Table 1, below). Many of these factors form the basis for breast cancer risk assessment tools. The common denominator for many of these risk factors is their effect on the level and duration of exposure to endogenous estrogen. Early menarche, nulliparity, and late menopause increase lifetime exposure to estrogen in premenopausal women, while obesity and hormone replacement therapy increase estrogen levels in postmenopausal women. One of the most widely studied risk factors in breast cancer is the use of exogenous hormones in the form of oral contraceptives (OCs) and hormone replacement therapy (HRT). The overall evidence suggests a modest 1.25 increased risk among current users of oral contraceptives. The risk appears to decrease with age and time from oral contraceptive discontinuation. Breast cancer risk returns to that of the average population after approximately 10 years following cessation of oral contraceptives. Consistent epidemiologic data support an increased risk of breast cancer incidence and mortality (2003) with the use of postmenopausal HRT. Risk is directly associated with length of exposure, with the greatest risk observed for the development of hormonally responsive lobular (relative risk [RR]=2.25, 95% confidence interval [CI]= 2.00-2.52), mixed ductal–lobular (RR=2.13, 95% CI= 1.68-2.70), and tubular cancers (RR=2.66, 95% CI= 2.16-3.28). The risk is greater in women taking combination estrogen plus progestin formulations compared to estrogen-only formulations (HR 0.77 for unopposed estrogen vs placebo), but missed statistical significance (p=0.06). Published results of a randomized trial, the Women’s Health Initiative (WHI), of estrogen-only and combination-HRT for the prevention of chronic disease indicate that the adverse outcomes associated with long-term use outweigh the potential disease prevention benefits particularly for women older than 65 years. Conversely, late menarche, anovulation, and early menopause (spontaneous or induced) are protective, owing to their effect on lowering endogenous estrogen levels or shortening the duration of estrogenic exposure. Table 1. Risk Factors for Breast Cancer Open table in new window [ CLOSE WINDOW ]
Table
There has been a concerted effort by several groups to develop multivariate methods to derive a Breast Cancer Risk Assessment Tool using sets of risk factors (genetic and other) that are informative for estimating the risk of breast cancer. Two types of risk models have been developed that are clinically relevant—those that estimate a woman’s absolute risk of developing breast cancer over time and those that determine the likelihood that an individual is a carrier of a BRCA1, BRCA2, or unknown gene mutation (ie, BRCA1/2 probability models). The most commonly used BRCAPRO model identifies approximately 50% of mutation-negative families but fails to screen 10% of mutation carriers. The BRCAPRO model, along with others (ie, Myriad I and II, Manchester, Breast and Ovarian Analysis of Disease Incidence and Carrier Estimation Algorithm[BOADICEA], and Ontario Family History Assessment Tool [FHAT]) were developed using mutation rates in Ashkenazi Jewish families and families of European descent but have recently been validated in African American and Hispanic populations. The U.S. Preventive Services Task Force (USPSTF) does not specifically endorse any of these genetic risk assessment models because of insufficient data to evaluate their applicability to asymptomatic, cancer-free women. The USPSTF does support the use of a greater than 10% risk probability for recommending further evaluation with an experienced genetic counselor for decisions regarding genetic testing. In contrast to BRCA probability tools, risk prediction models are designed to derive individual risk estimates for the development of breast cancer over time. The Gail Model was originally developed in 1989 from data derived from the Breast Cancer Detection and Demonstration Project (BCDDP). It was developed to estimate the probability of developing breast cancer over a defined age interval and was originally intended to improve screening guidelines. The model was subsequently revised (Gail Model 2) and validated to predict risk of invasive breast cancer including information on the history of first-degree affected family members. The Gail Model 2 has been used extensively in clinical practice and has served as the basis of eligibility for a number of the breast cancer prevention trials. At present, the U.S. FDA guidelines use the National Surgical Adjuvant Breast and Bowel Project’s (NSABP) modified Gail model as the basis for eligibility for the prophylactic use of tamoxifen. Tamoxifen is approved for women aged 35 years and older who have a 5-year Gail risk of breast cancer of 1.67% or more. The Gail Model 2 also forms the basis of the U.S. National Cancer Institute’s Breast Cancer Risk Assessment Tool. The Gail Model 2 is most accurate for non-Hispanic White women who receive annual mammograms, but the model tends to overestimate risk in younger women who do not receive annual mammograms. The model also demonstrates reduced accuracy in populations with demographics (age, race, screening habits) that differ from the population on which it was built. At the individual level, the model lacks adequate discrimination in predicting risk and has been challenged on its generalizability across populations. To address concerns regarding applicability of the Gail Model to African American women, Gail and colleagues have derived a CARE Model using data from a large case control study of African American women participating in the Women’s Contraceptive and Reproductive Experiences (CARE) Study. The CARE Model demonstrated high concordance between the numbers of breast cancer predicted and the number of breast cancers observed among African American women when validated in the WHI cohort. Improvements in risk prediction and clinical tools are likely to emerge in the next few years with the addition of such factors as breast density, mammographic density change across exams, use of HRT, and a variety of other factors such as weight, age at birth of first live child, and number of first-degree relatives with breast cancer. Going forward, it is likely that there will be models specifically for risks of premenopausal versus postmenopausal cancers and for specific breast cancer subtypes (luminal versus basal). Genetic factors While 20-30% of women with breast cancer have at least one relative with a history of breast cancer, only 5-10% of women with breast cancer have an identifiable hereditary predisposition. BRCA1 and BRCA2 mutations are responsible for 3-8% of all cases of breast cancer and 15-20% of familial cases. Rare mutations are seen in the PTEN, TP53, MLH1, MLH2, and STK11 genes. The BRCA1 and BRCA2 gene mutations, on chromosome 17 and 13, respectively, account for the majority of autosomal dominant inherited breast cancers. Both genes are believed to be tumor suppressor genes whose products are involved with maintaining DNA integrity and transcriptional regulation. Specifically, BRCA1 mutations are seen in 7% of families with multiple breast cancers and 40% of families with breast and ovarian cancer. People with a BRCA1 mutation have a lifetime risk of 40% for developing ovarian cancer and are also at a higher risk of colon cancer and prostate cancer. Breast cancer that develops in BRCA1 mutation carriers are more likely to be high-grade, and ER, PR, and HER-2/neu negative (triple negative) or basal-like subtype. BRCA2 mutations are identified in 10-20% of families at high risk for breast and ovarian cancers and in only 2.7% of women with early-onset breast cancer. Women with a BRCA2 mutation have approximately 10% lifetime risk of ovarian cancer. BRCA2 mutation carriers who develop breast cancer are more likely to have a high grade, ER+/PR+, and HER-2/neu negative cancer (luminal type). BRCA2 is also a risk factor for male breast cancer. Other cancers associated with BRCA2 mutations include prostate, pancreatic, fallopian tube, bladder, non-Hodgkin lymphoma, and basal cell carcinoma. Li-Fraumeni syndrome, caused by TP53 mutations , is associated with multiple cancers, including the SBLLA syndrome (sarcoma, breast and brain tumors, leukemia, and laryngeal and lung cancer). Cancer susceptibility is transmitted in an autosomal dominant pattern, with a lifetime risk of breast cancer of 90%. Li-Fraumeni syndrome is responsible for approximately 1% of cases of familial breast cancer. Bilateral breast cancer is noted in up to 25% of patients. Cowden disease is a rare genetic syndrome caused by PTEN mutations. It is associated with intestinal hamartoma, cutaneous lesions, and thyroid cancer. The prevalence rate of breast cancer in women with this disease is approximately 30%. Benign mammary abnormalities (eg, fibroadenomas, fibrocystic lesions, ductal epithelial hyperplasia, and nipple malformations) are also common. Other rare genetic disorders, such as Peutz-Jeghers and hereditary nonpolyposis colorectal carcinoma (HNPCC), are associated with an increased risk of breast cancer. Early detection remains the primary defense available to patients in preventing the development of life-threatening breast cancer. Breast tumors that are smaller or nonpalpable are more treatable when detected and thus have a more favorable prognosis. The survival benefit of early detection with mammography screening has been demonstrated. Therefore, early detection is widely endorsed by organizations that issue clinical recommendations for breast cancer care. For women younger than 40 years, monthly breast self-examination practices and clinical breast exams every 3 years are recommended, beginning at age 20 years. Both breast self-examination and clinical breast examination involve inexpensive and noninvasive procedures for the regular examination of breasts (ie, monthly for breast self-examination and annually for clinical breast examination). Evidence supporting the effectiveness of breast self-examination and clinical breast examination are controversial and largely inferred. Mammography Mammography has been demonstrated to be an effective tool for the prevention of advanced breast cancer in women at average risk. Mammography is currently the best available population-based method to detect breast cancer at an early stage when treatment is most effective. Mammography often reveals a lesion before it is palpable by clinical breast examination and, on average, 1-2 years before noted by breast self-examination. Recent advances in mammography include the development of digital mammography and the increased use of computer-aided diagnosis (CAD) systems. CAD systems have been developed to help the radiologist identify mammographic abnormalities. Digital mammography allows the image to be recorded and stored. Using computer technology, digital mammogram images can be magnified and the image modified to improve evaluation of specific areas in question. The USPSTF estimates the benefit of mammography in women aged 50-74 years to be a 30% reduction in risk of death from breast cancer. For women aged 40-49 years, the risk of death is decreased by 17%. Although mammography guidelines have been in place for over 30 years, 20-30% of women still do not undergo screening as indicated. The two most significant factors for a woman to undergo mammography are physician recommendation and access to health insurance. Non-white women and those of lower socioeconomic status remain less likely to obtain mammography services and more likely to present with life-threatening, advanced-stage disease. Alternative screening modalities and future directions While mammography remains the most cost-effective approach for breast cancer screening, the sensitivity (67.8%) and specificity (75%) are not ideal. As reported, mammography combined with clinical breast examination slightly improves sensitivity (77.4%) with a modest reduction in specificity (72%). Comparisons between recently introduced digital mammography and screen-film mammography suggest that the sensitivity of full-field digital mammography is superior to screen film mammography in certain subsets of women. For example, digital mammography demonstrates improved detection rates for younger women and for women with more dense breasts. Improved imaging modalities with greater sensitivity are of particular benefit for women at the highest risk and for women whose breast images are difficult to interpret. Ultrasound has become a widely available and useful adjunct to mammography in the clinical setting. Ultrasound is generally used to assist the clinical examination of a suspicious lesion detected via mammogram or physical examination. As a screening device, the ultrasound is limited by a number of factors, but most notably by the failure to detect microcalcifications and poor specificity (34%). In an effort to overcome the limitations of mammography and ultrasound, magnetic resonance imaging (MRI) has been explored as a modality for detecting breast cancer in women at high risk and in younger women. A combination of T-1, T-2, and 3-D contrast-enhanced MRI techniques has been found to be highly sensitive (approximating 99% when combined with mammogram and clinical breast examination) to malignant changes in the breast. MRI has been demonstrated to be an important adjunct screening tool for women with BRCA1 or BRCA2 mutations identifying cancers at earlier stages. However, breast MRI has limited use as a general screening tool with a 10-fold higher cost than mammography and poor specificity (26%), resulting in significantly more false-positive reads that generate significant additional diagnostic costs and procedures. Below are the criteria for using breast MRI screening per the American Cancer Society (ACS).6
The American Cancer Society does not recommend the use of breast MRI in women who have less than 15% lifetime risk. Among those with average risk, a combination of clinical breast examinations and yearly mammograms is recommended. Two selective estrogen receptor modulators (SERMs), tamoxifen and raloxifene, are approved for reduction of breast cancer risk in high-risk women. Two National Surgical Adjuvant Breast and Bowel Project (NSABP P1 and P2) trials showed that tamoxifen reduced the risk of ductal carcinoma in situ (DCIS) and invasive breast cancer by 30-50%. In the NSABP P2 prevention trial, raloxifene was as effective as tamoxifen in reducing the risk of invasive breast cancer but was 30% less effective than tamoxifen in reducing the risk of DCIS. The American Society of Clinical Oncology (ACOG) has updated their practice guidelines regarding pharmacologic intervention (eg, tamoxifen, raloxifene, aromatase inhibition) for breast cancer risk reduction.7 Some of the highlights of the expert panel's literature review are as follows:
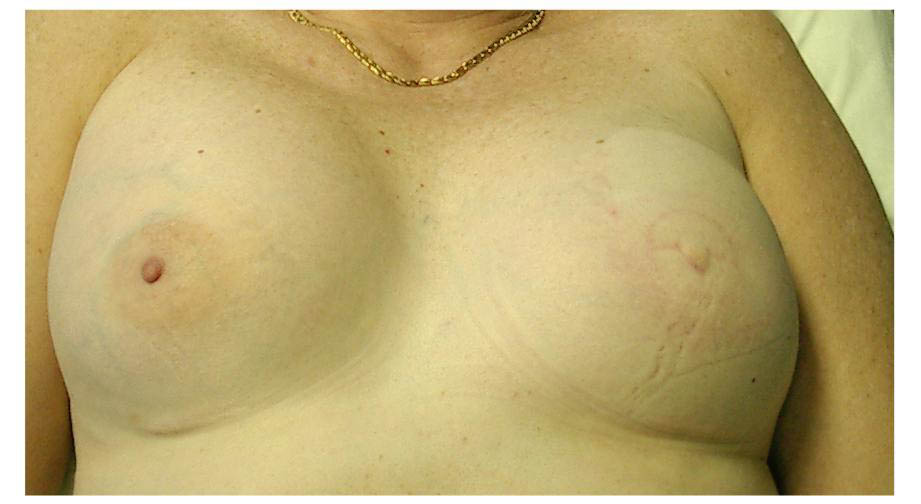
PresentationBreast cancer is often first detected as an abnormality on a mammogram before it is felt by the patient or health care provider. Mammographic features suggestive of malignancy include asymmetry, microcalcifications, a mass, or architectural distortion. If any of these features are identified, a diagnostic mammogram along with a breast ultrasound should be performed prior to obtaining a biopsy. In certain cases, a breast MRI may be warranted. Larger tumors may present as a painless mass. Only 5% of patients with a malignant mass present with breast pain. Other symptoms include immobility, skin changes (ie, thickening, swelling, redness) or nipple abnormalities (ie, ulceration, retraction, spontaneous bloody discharge). .
|