TULAREMIA
(FRANCISELLA TULARENSIS INFECTIONS)
Etiology and Epidemiology
Tularemia is a zoonotic infectious disease caused by Francisella tularensis, a pleomorphic Gram-negative coccobacillus found in many species of mammals, most important, lagomorphs (rabbits and hares) and rodents, and in their immediate environments. The bacteria are highly infectious, can be transmitted in many ways, and cause at least eight different patterns of disease.
Tularemia occurs solely in temperate and cold regions of the Northern Hemisphere. The most common form in the United States is ulcero-glandular disease in which organisms are inoculated directly into the skin by minor trauma or by bites of infected arthropods that maintain the enzootic cycle. Before 1950, most U.S. infections occurred in hunters who handled infected rabbits and hares. Two incidence peaks each year corresponded with summer and winter hunting seasons. Currently, 100 to 200 U.S. cases occur each year, mostly in Arkansas, Missouri, Oklahoma, and South Dakota, with transmission of the organism largely via tick bites. The most common tick vectors are Dermacentor sp., Amblyomma americanum, and, in Europe, Ixodes sp.
Clinical Findings
HISTORY
Duration of incubation varies with size of inoculum, ranging from 2 to 10 days. All forms of tularemia present as a sudden flu-like illness characterized by fever, headache, malaise, and myalgias.
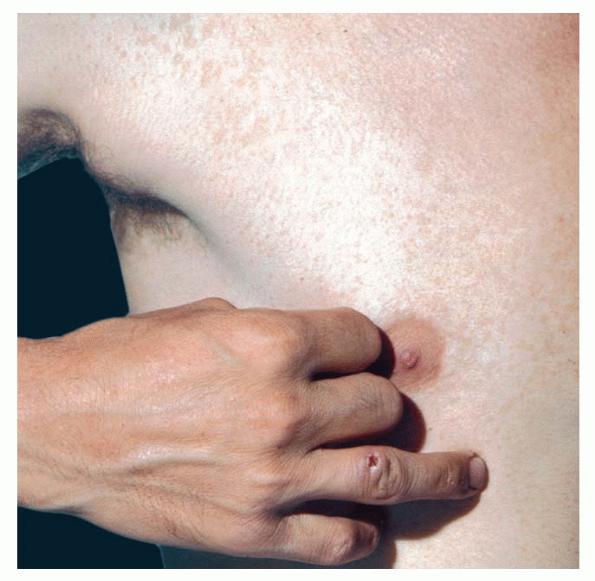
CUTANEOUS LESIONS
In ulcero-glandular tularemia, a painful red papule appears at the inoculation site . It enlarges rapidly and evolves into a necrotic chancriform ulcer often covered by a black eschar. Regional lymph nodes are large and tender. Bacteremia may cause sepsis and virulent pneumonia.
RELATED PHYSICAL FINDINGS
In oculoglandular tularemia, organisms are introduced directly into the conjunctivae, for example, after handling an infected tick or rabbit. This causes purulent conjunctivitis with pain, edema, and local adenopathy. In a recent outbreak in Bulgaria, more than 90 percent of cases were oropharyngeal, reflecting transmission via contaminated well water. Swallowing the organism may cause ulcerative pharyngotonsillitis with cervical adenopathy or may cause “typhoidal” tularemia. Pulmonary tularemia may be primary (i.e., due to inhalation of organisms) but is more often due to bacteremic spread from another focus.
TULAREMIA AT A GLANCE
· Caused by Francisella tularensis, a Gram-negative coccobacillus found in rabbits, rodents, other mammals, and their immediate environments in temperate and cold regions of North America.
· Has diverse clinical presentations related to route of transmission. Ulcero-glandular disease after tick bites is most common.
· Bacteria are easily aerosolized and highly infectious in small inocula; therefore, tularemia poses risks of laboratory accidents or use as a bioweapon.
Histopathology
The pathogen survives intracellularly in phagocytes, and small granulomas develop in lymph nodes, liver, and spleen. Some lesions may caseate and progress to frank abscess formation. Hepatic granulomas may resemble tuberculosis or brucellosis.
Treatment
A presumptive diagnosis of tularemia on clinical and epidemiologic grounds is sufficient to initiate treatment while awaiting serologic confirmation . Streptomycin is effective against all forms of tularemia when started promptly. Gentamicin appears to be an acceptable alternative. Patients improve within 24 to 48 hours, but treatment should continue for at least 7 to 10 afebrile days. Tetracycline and chloramphenicol are other acceptable alternatives but should be given for longer periods to reduce the risk of relapse.