|
Acarid mites produce several skin manifestations in humans, the most common one represented by scabies, which is caused by the eight-legged itch mite Sarcoptes scabiei var. nominis, also referred to as s. sarcoptes scabiei. Animal pathogenic mites also affect the skin, although only transiently because the mites do not survive for an extended period of time .
|
|
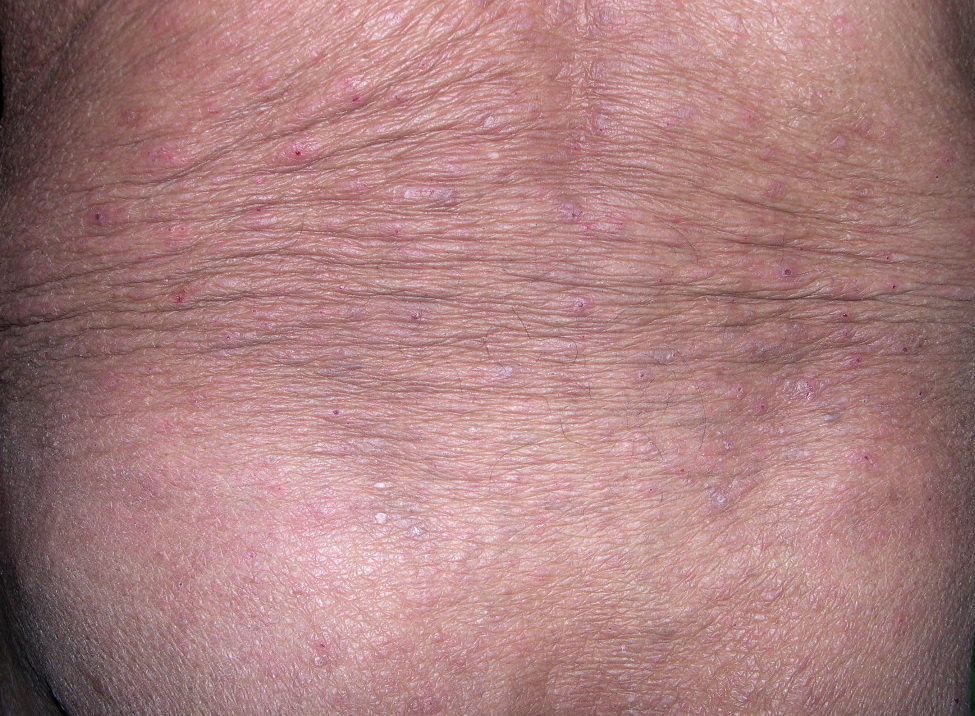
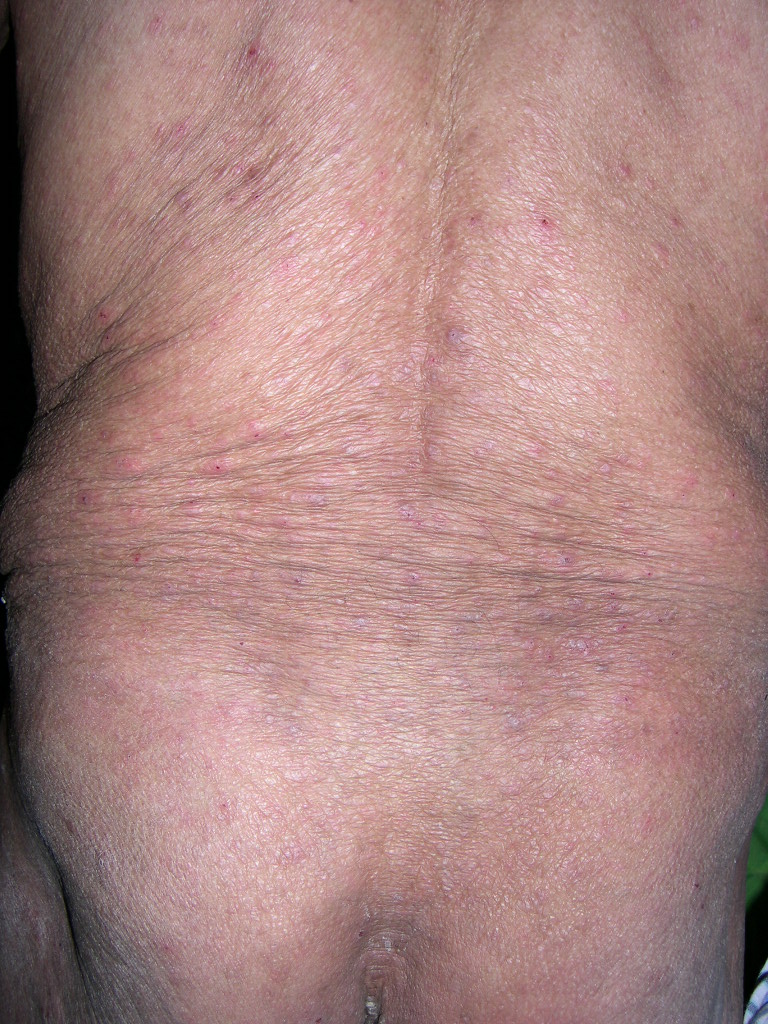
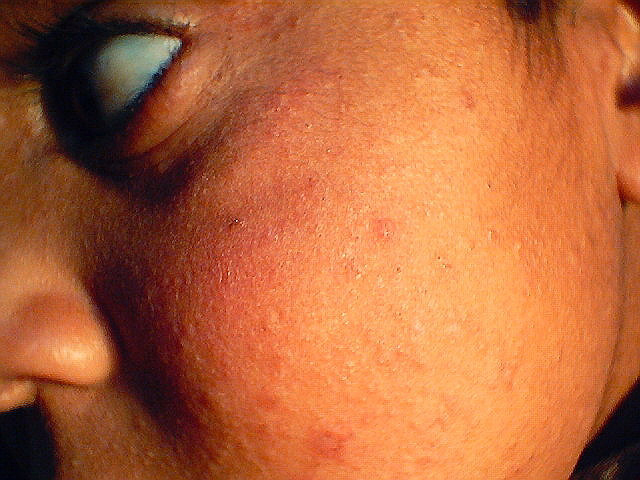
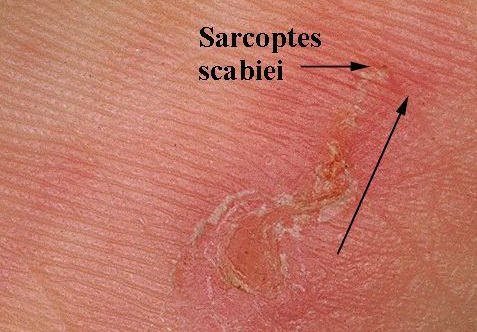
Burrows are the pathognomonic lesions of scabies and are found mostly in the florid, papulovesicular type of sarcoptic acariasis . They are produced by female mites and occur mainly on the palms and plantae, the palmar and lateral aspects of the fingers and toes, the interdigital spaces, the flexor surfaces of the wrists, the nipples of women, the genitals of men, and, to a lesser extent, on the buttocks and axillae. Characteristically, the head is spared, except in newborns and infants . The burrows appear as fine, tortuous, blackish threads a few millimeters long. A vesicle may be visible near the blind end of the burrow. The mite is situated in this vesicle and may be visible as a tiny gray speck by dermatoscopy. Although pathognomonic, the burrow is not the most common lesion seen in scabies. Small, erythematous, often excoriated papules are more frequent .
|
|
In some patients, itching nodules persist for several months after successful treatment, and therefore are named
|
|
nodular scabies or persistent scabietic nodules. They are found most commonly on the scrotum and are believed to result from a prolonged response to persistent scabies antigens .
|
|
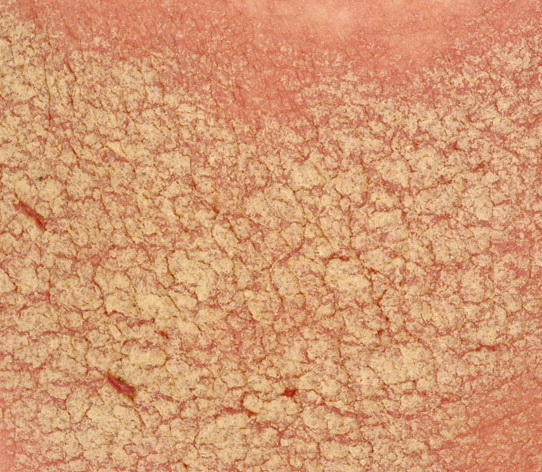
In a third, rare variant, the so-called Norwegian scabies or crusted scabies, innumerable mites are present. Patients with this variant show widespread erythema, hyperkeratosis, crusting, nail thickening, and subungual hyperkeratosis but no obvious burrows.
|
|
Histopathology.
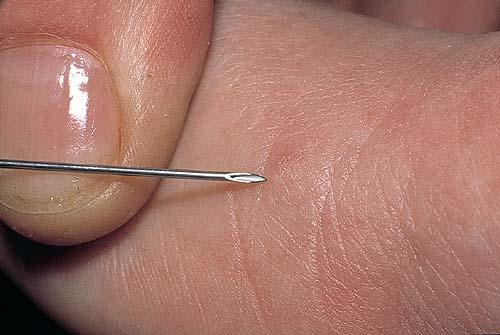
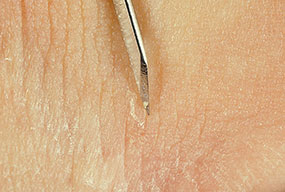
A definitive diagnosis of scabies can be made only by demonstration of the mite or its products. A very superficial epidermal shave biopsy of an early papule or, preferably, of an entire burrow may be carried out with a #15 scalpel blade . Local anesthesia is not required. The biopsy specimen is placed on a glass slide, and a drop of immersion oil and then a cover slip are placed on top of it . This technique yields a higher percentage of positive preparations than the often performed mere scraping of a suspicious lesion with a scalpel blade.
|
|
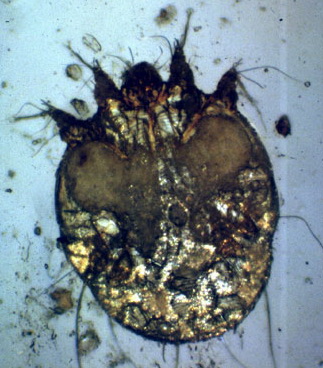
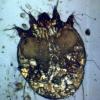
Histologic examination of a specimen containing a burrow reveals that the burrow in almost its entire length is located within the horny layer . Only the extreme, blind end of the burrow, where the female mite is situated, extends into the stratum malpighii . The mite has a rounded body and measures about 350 to 450 IJm in length and 250 to 350 IJm in width .
|
|
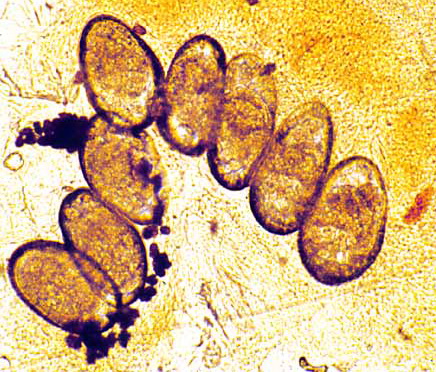
In the papulovesicular form of scabies, spongiosis is present in the stratum malpighii near the mite to such an extent that formation of a vesicle is often the result. Even if no mite is found in the sections, the presence of eggs containing larvae, of egg shells, or of fecal deposits (scyballa) within the stratum corneum is indicative of scabies . The dermal infiltrate in sections containing mites shows varying numbers of eosinophils.
|
|
In nodular or persistent nodular scabies, there is a dense, chronic inflammatory, often pseudolymphomatous infiltrate in which many eosinophils may be present. Vasculitis is considered by some as being frequent (49) but by others as representing a rather uncommon event . These different findings may be related to the duration of the scabietic nodules and the timing of the biopsy . The nodules are rich in indeterminate cells, sometimes misleading to the diagnosis of Langerhans cell histiocytosis based on light microscopy and immunophenotyping alone (50). Atypical mononuclear, CD30+ cells may be found (51), and in some instances, the nodules show, as in persistent arthropod bites or stings (see later discussion), a histologic picture resembling that of lymphoma . Viable mites are hardly ever found in the nodules. However, mite parts are seen in up to 22% of cases .
|
|
In Norwegian scabies, the thickened horny layer is riddled with innumerable mites, so that nearly every section shows several parasites .
|
|
Pathogenesis. Earlier scanning electron microscope studies revealed the keratinocytes around the burrow to be compacted, indicating that the mite physically forces its way in between the keratinocytes rather than chewing a passage (48). More recent studies, however, also using transmission electron microscopy, have found that the secretion of cytolytic substances by the mite as a contributing factor in advancing the parasite body through the skin in addition to mere compression (53). The cellular damage was greatest around the body, especially the mite capitulum.
|
                                                                   
|