Constricting Bands Ainhum and
Pseudoainhum
▪ AINHUM AND PSEUDOAINHUM
Constricting bands are classified as ainhum and pseudoainhum. Ainhum is the development of constricting bands around toes in underdeveloped countries of Africa and may ultimately result in autoamputation. In the African Yorub language, ainhum means “to saw or file,” and in the Brazilian patois it means “fissure.”1 In the remainder of the world, constricting bands that mimic ainhum are termed pseudoainhum.
▪ EPIDEMIOLOGY
Ainhum (dactylolysis spontanea) is traditionally a disease of middle-aged African males accustomed to going barefoot. In tropic and sub-tropic climates its incidence has been reported as between 0.015 percent and 2.0 percent of the population. This same condition is rarely seen throughout the rest of the world. Occasional isolated cases have been reported in North America. Pseudoainhum of all types is very rare.
▪ ETIOLOGY AND PATHOGENESIS
The pathogenesis of ainhum has not been clearly elucidated. Chronic trauma, infection, hyperkeratosis, decreased vascular supply, and impaired sensation may produce excessive fibroplasia in a susceptible host. Dent et al. described impaired blood supply to the foot proximal to the groove at the plantar digital junction. Poor perfusion was the result of attenuation of the posterior tibial artery and absence of the plantar arterial arch, which led to abnormal healing after mechanical trauma. Ainhum has also been blamed on rotational stress applied to the bare, mechanically unstable foot.
There are three pathophysiologic categories of pseudoainhum: (1) congenital constricting bands caused by the umbilical cord; (2) constriction due to external forces, such as hairs or threads, which are generally factitial; and (3) constricting bands secondary to other diseases. The latter may be hereditary or nonhereditary. Hereditary causes include pachyonychia congenita, mal de Meleda, mutilating keratoderma, and psoriasis. Non-hereditary causes include vascular anomalies as seen in Raynaud disease, diabetes mellitus, linear scleroderma, and systemic sclerosis. Sensory changes associated with leprosy, tertiary syphilis, syringomyelia, and spinal cord tumors as well as trauma resulting in scar formation from burns, frostbite, and physical trauma can also cause constricting bands to form. When pseudoainhum is associated with chronic trauma and infection of the extremities, the pathophysiology may be identical to that of true ainhum.
CONSTRICTING BANDS AT A GLANCE
· Constricting bands (ainhum and pseudoainhum) cause amputation (autoamputation) of digits.
· Ainhum is a constricting band around a digit and is most common in the tropics and sub-tropics.
· It is most common around the fifth toe of people walking barefoot.
· Pseudoainhum constrictions mimic ainhum clinically and are more common in the developed world. They are caused by the following:
o Amniotic bands
o Constrictions associated with keratotic disorders, infections, and trauma
o Constriction by external materials such as hairs and threads
· Treatment is removal of the foreign strands or surgical intervention.
▪ CLINICAL FINDINGS
Ainhum usually affects the fifth toe . It may be unilateral, but 75 percent of cases are bilateral. In early lesions, a groove or sulcus appears at the plantar junction of the toe and the sole. As this sulcus deepens, edema develops distally, and roentgenographic examination shows resorption of the underlying bone and ultimately autoamputation.
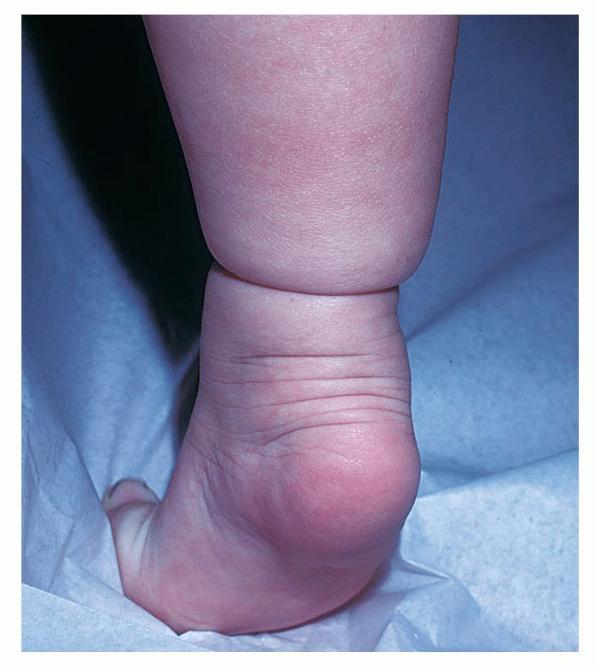
Congenital constricting bands (Streeter's bands) usually involve more than one part of the body . They frequently encircle large structures such as limbs or even the trunk . They persist throughout life and interfere with normal growth of the involved segment unless surgically treated.7 In more than 50 percent of cases, they are associated with other congenital anomalies, usually syndactyly or clubfoot when constricting bands are found on the feet.
Artifactual pseudoainhum may prove to be a most challenging diagnosis. Strands of hair, fibers, or threads may be intentionally wrapped around digits or other body parts such as a nipple or penis.
This phenomenon is most commonly encountered in children but can occur in mentally ill adults. Because of soft-tissue swelling, the ligating band may not be visible and the true cause of the condition may not be immediately recognized.
Acquired constricting bands are associated with a variety of medical and dermatologic conditions. In general, pseudoainhum is more likely to involve any of the toes or even the hands. In children, when chronic dermatophyte infection is identified and appropriately treated, complete reversal of the constriction may occur. Severe hyperkeratosis as occurs in Vohwinkel syndrome or keratoderma hereditarium mutilans may show constricting bands due to palmar and plantar hyperkeratoses as well as starfish-like and linear keratoses . Pseudoainhum may occur in severe psoriasis of the digits .
The pathology of ainhum and pseudoainhum is similar, with the presence of fibrotic bands resembling scar tissue. The bands in ainhum usually extend deep into the subcutaneous layers and may impinge on underlying skeletal and vascular structures. In addition, moderate inflammation and epidermal or verrucous hyperplasia may be present. In pseudoainhum the bands tend to be more superficial. Also, in pseudoainhum there may be histologic clues to the associated disorder, such as dermatophytosis, foreign bodies, or distinct patterns of keratinization.
▪ COMPLICATIONS
The constricting bands of both ainhum and pseudoainhum ultimately produce a dangling, twisted digit, which can become gangrenous or infected. When this tenuous connection leads to necrosis, autoamputation occurs.
▪ PROGNOSIS AND CLINICAL COURSE
Diseases caused by constricting bands proceed slowly and often painfully over many years, eventuating in autoamputation in severe cases.
▪ TREATMENT
Surgery is the mainstay of therapy, and early intervention is important. In most cases of ainhum, prompt amputation may allow the patient to escape pain and infection. Early cases of ainhum or pseudoainhum may respond to conservative plastic repair with a Z-plasty or similar relaxing closure that prevents further disease progression and damage to underlying structures.10
Impending amputation in Vohwinkel syndrome can sometimes be aborted by therapy with oral etretinate . When chronic fungal or bacterial infections are diagnosed in the early phase of band formation, treatment may reverse the threat to the digit. Other predisposing causes or underlying diseases should be treated aggressively in the hope of forestalling progression.
▪ PREVENTION
Ainhum is rarely seen in people whose feet are protected by wearing shoes. Congenital pseudoainhum cannot be prevented and can lead to serious birth defects (see eFig. 66-3.2 in on-line edition). Psychological counseling may prevent recurrences of pseudoainhum in patients with factitial disease. Control of the underlying disease process may delay progression or prevent recurrence in pseudoainhum of the acquired type.