| Perioral dermatitis = التهاب الجلد ماحول الفم |
|
|
Perioral Dermatitis
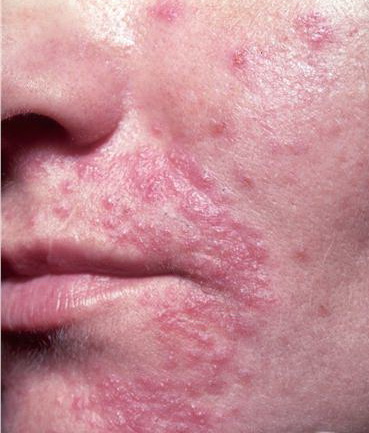
Perioral dermatitis is characterized by small discrete papules and pustules in a periorificial distribution, predominantly around the mouth. Although initially described as an eruption in young women 15 to 25 years of age, perioral dermatitis is now recognized to occur occasionally in children as well. A subset of perioral dermatitis shows granulomas when lesional skin is examined histologically. Several names have been used to describe this granulomatous form of perioral dermatitis, including granulomatous perioral dermatitis, facial Afro-Caribbean childhood eruption, and granulomatous periorificial dermatitis. HISTORICAL ASPECTS EPIDEMIOLOGY Unlike adult perioral dermatitis, which affects predominantly women, pediatric perioral dermatitis is seen equally in boys and girls and among those of different races. The granulomatous form of perioral dermatitis has been reported mostly in children of prepubertal age.An increased prevalence in African American children has been reported, but more recent reviews do not support this finding. ETIOLOGY AND PATHOGENESIS The relationship of perioral dermatitis to the misuse of potent topical corticosteroids (fluorinated or non-fluorinated) has been well established.11 Patients often reveal a history of an acute steroid-responsive eruption around the mouth, nose, and/or eyes that worsens when the topical corticosteroid is discontinued. Dependency
PERIORAL DERMATITIS AT A GLANCE
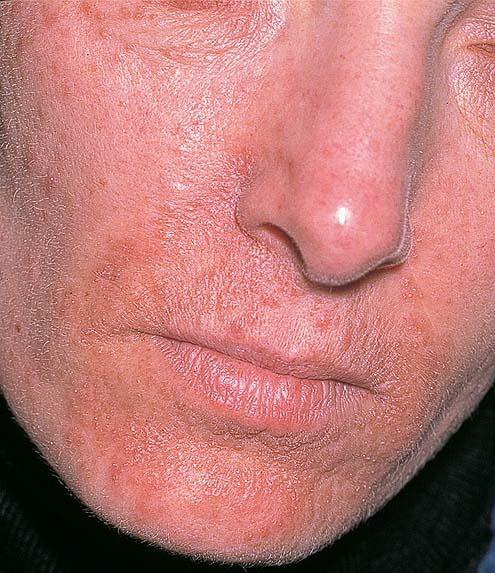
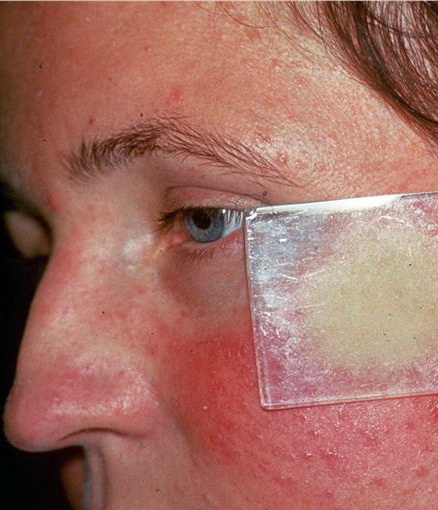
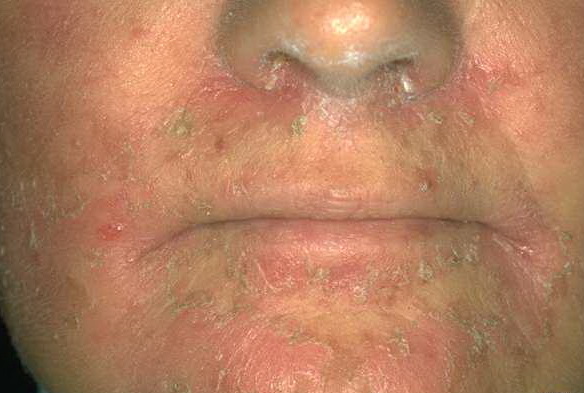
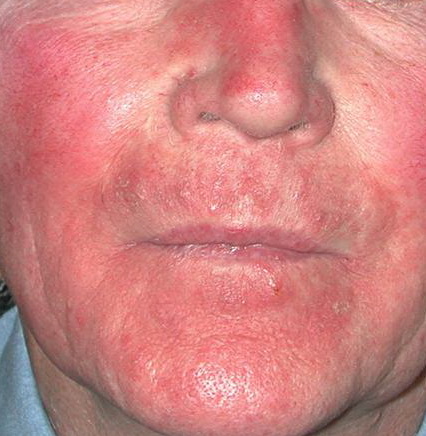
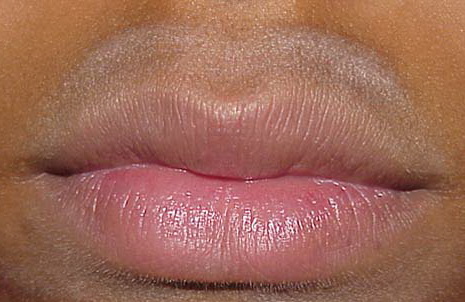
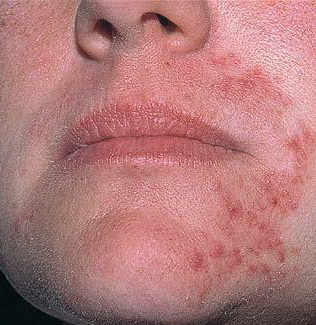
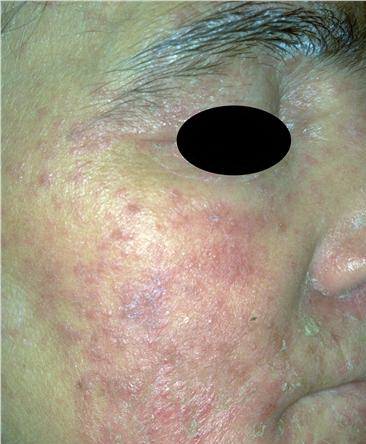
In the past, authors have considered the relationship of periorificial dermatitis to acne rosacea; however, the clinical features are distinct (see Differential Diagnosis). The histopathologic findings are variable. The pathology described in 26 patients showed spongiotic changes in the external root sheaths of the follicles without similarity to rosacea. However, granulomatous perioral dermatitis shows the histopathologic changes of follicular hyperkeratosis, edema and vasodilation of the papillary dermis, perivascular and parafollicular infiltrates of lymphocytes, histiocytes, and polymorphonuclear leukocytes with occasional epithelioid granulomas and giant cells, similar to the histopathologic changes in acne rosacea.4,15 CLINICAL FINDINGS The primary lesions of perioral dermatitis are discrete and grouped erythematous papules, vesicles, and pustules . The lesions are often symmetric but may be unilateral and appear in the perioral, perinasal, and periorbital regions . A background of erythema and scale may occur. A distinct 5-mm clear zone at the vermilion edge is well described . The granulomatous variant of perioral dermatitis presents with small flesh-colored, erythematous, or yellow-brown papules, some with confluence, and shares the distribution of perioral dermatitis in adults. In addition, lesions have been reported to appear on the ears, scalp, trunk, labia majora, and extremities. Rarely an associated burning sensation or itching is reported, and intolerance to moisturizers and other topical products is described. In a few cases of granulomatous perioral dermatitis an associated blepharitis or conjunctivitis has occurred.10 DIFFERENTIAL DIAGNOSIS The differential diagnosis of perioral dermatitis in young adults includes acne rosacea, acne vulgaris, seborrheic dermatitis, allergic and irritant contact dermatitis, Gram-negative folliculitis, angular cheilitis, and lip-licking cheilitis. In children, the diagnosis of irritant contact dermatitis to saliva from the use of a pacifier, sucking of the thumb or fingers, and messy eating is common and should be considered as well. Infection with D. folliculorum can present like perioral dermatitis but with atypical pustules and symptoms of pruritus,19 or as a perioral dermatitis-like eruption in the immunocompromised host.13 Differential Diagnosis of Perioral Dermatitis
Granulomatous rosacea, sarcoidosis, lupus miliaris disseminatus faciei, fungal or mycobacterial infection, familial juvenile systemic granulomatosis (Blau syndrome), and benign cephalic histiocytosis should be considered in the differential diagnosis of granulomatous perioral dermatitis. Granulomatous perioral dermatitis lacks systemic symptoms. A thorough history and physical examination, review of symptoms, chest radiography, ophthalmologic examination, and histopathologic evaluation of skin biopsy specimen can differentiate these disorders when indicated.10 Sarcoidosis in young children is rare and often accompanied by systemic signs and symptoms, particularly weight loss, fatigue, joint pains, lymphadenopathy, and uveitis. At least some of the reported cases of sarcoidosis in young children represent Blau syndrome with underlying mutations in CARD15/NOD2 . Treatment for Perioral Dermatitis
COMPLICATIONS The majority of cases of perioral dermatitis and granulomatous perioral dermatitis resolve without sequelae or relapse. However, there are rare reports of scarring. PROGNOSIS AND CLINICAL COURSE Perioral dermatitis is usually a self-limited disorder that evolves during a few weeks and resolves over months or rarely years. If treated with topical corticosteroids alone, recurrent episodes on withdrawal of therapy or with continuing therapy are typical. With appropriate treatments the condition resolves with rare recurrences. TREATMENT If topical corticosteroids are being used, they should be discontinued. If fluorinated corticosteroids are being applied, initial substitution with a low-potency hydrocortisone cream may minimize a flare of the dermatitis. Patients should be educated about the link between application of topical corticosteroids and exacerbation of the dermatitis. In most cases, treatment includes oral tetracycline, doxycycline, or minocycline, for a course of 8 to 10 weeks, including a taper over the last 2 to 4 weeks. Severe cases may respond better to minocycline or doxycycline or high-dose tetracycline therapy. In children under 8 years of age, nursing mothers, or tetracycline-allergic patients, oral erythromycin is recommended. Not uncommonly, patients require continued low-dose systemic antibiotic therapy for months or sometimes years to maintain control. Topical antibiotic therapy, most commonly with topical metronidazole, should be initiated concurrently with the systemic antibiotic. For milder cases, initial application of topical metronidazole alone may suffice. Other options include topical clindamycin or erythromycin, topical sulfurbased preparations, and topical azelaic acid.Reports of successful use of topical calcineurin inhibitors exist; however, caution is advised given the occasional reports of granulomatous eruptions after the use of these preparations. Photodynamic therapy with topical 5-aminolevulinic acid has shown promise for treating perioral dermatitis as well. PREVENTION The only factor widely accepted to predispose to perioral dermatitis is the use of topical corticosteroid preparations, and avoidance of these products may prevent the eruption in some cases.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||