Pediculosis Pubis (Pubic Lice)
EPIDEMIOLOGY
Most often pubic lice are a sexually transmitted disease and approximately 30 percent of patients have another concurrent sexually transmitted disease. Fomite transmission has also been documented to occur from contaminated clothing, towels, or bedding.
ETIOLOGY AND PATHOGENESIS
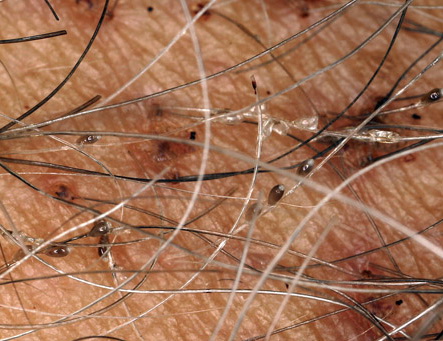
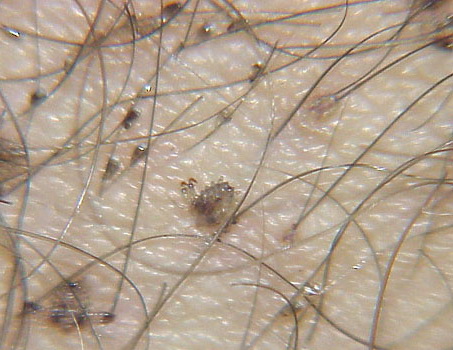
Pubic lice or Pthirus pubis belongs to a separate genus and species in the family Pthiridae. The common term crab louse is an excellent description for the distinct morphology, the body being somewhat rounded like that of a crab. Pubic lice range from 0.8 to 1.2 mm in length. With the use of serrated edges on the first claw, pubic lice are able to ambulate up to 10 cm/day. As suggested by its name, this louse is most commonly found in the pubic hair, although in hirsute individuals the short hairs of the thighs, trunk, and perianal area may also be involved. Occasionally, the beard, moustache, and even eyelashes may be involved. Infestation of the eyelashes and periphery of the scalp occur mainly in children, probably a result of contact with an infested parent. Meinking and Taplin reported as much as 60 percent of a homeless population had crab lice in areas of the body besides the pubic hair. The crab louse has a lifespan of 2 weeks and during this time the female louse can produce around 25 ova. The adult crab louse can survive away from the human host for up to 36 hours.
CLINICAL FINDINGS
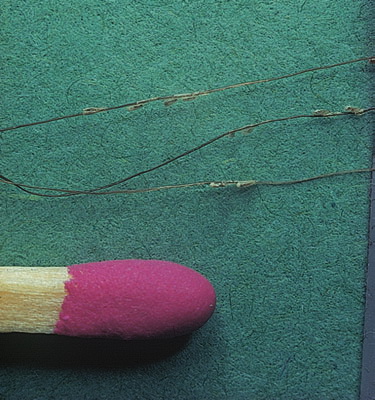
As with all pediculoses, patients typically present with pruritus. Maculae coeruleae (sky-blue macules), most commonly found on thighs or trunk, may be present as in pediculosis corporis . The diagnosis is most frequently made by the patient him- or herself, often identifying the louse in the pubic area. Infested patients reportedly have an average of 10 to 25 or more adult organisms on the body. When the lice themselves cannot be found, nits may be identified near the base of the hair (Fig. 208-9). As in pediculosis capitis, the duration of infestation can be approximated by the distance of the nit from the skin surface. The diagnosis is confirmed by microscopic examination of the plucked hair to identify the nits. Empty nits may indicate a prior infestation.
Secondary infection because of excoriation can lead to local lymphadenitis and fever.
PROGNOSIS AND CLINICAL COURSE
Untreated, pediculosis pubis infestations may persist for years.
TREATMENT
Topical therapy is much the same as that for pediculosis capitis. The preparation should be applied to the infested area, paying particular attention to the pubic and perianal regions and adjacent hairy areas. A common cause of failure is treating only the pubic area in hairy individuals: The pediculicide should be applied to the thighs, trunk, and axillary regions because the mite can infest these areas as well. Sexual contacts should be treated simultaneously,
but other family members need not be treated if there is no evidence of infestation
Differential Diagnosis of Pubic Lice
Most Likely
- · Extensive excoriations
- · Scabies infestation
- · Contact dermatitis
Consider
- o Trichosporon cutaneum
- · Trichomycosis pubis
- · Hair casts (pseudonits
Always Rule Out
Treatment for Pubic Lice
|
TREATMENT
|
ADMINISTRATION
|
COMMENTS
|
|
Synergized pyrethrins and permethrin 1% shampoos
|
Topically 10 min; repeat in 7-10 days
|
Available over-the-counter
|
|
Permethrin 5% cream
|
Topically 8-12 h; repeat in 7-10 days
|
Currently treatment of choice
|
|
Lindane shampoo 1%
|
Topically 5 min
|
Risk of central nervous system toxicity
|
|
Occlusive agent (Vaseline)
|
Applied to eyelashes twice daily for 8 days; manual removal of nits
|
None
|
|
Ivermectin, oral
|
250 µg/kg dose given 7 to 10 days apart demonstrated effective for eyelash involvement
|
Risk profile, see Box 208-4
|
TREATMENT FAILURE
Treatment failure is usually a result of failure to follow instructions, neglecting to treat sexual contacts, or re-infestation. Patients with human immunodeficiency virus/acquired immunodeficiency syndrome tend to have more severe infestations with pediculosis pubis and to be unresponsive to conventional therapy. Persistent itching may be caused by irritation from the pediculicide (usually because of overuse) or patient anxiety. Parasitophobia is fairly common after infestation and is difficult to treat.