▪ NOCARDIOSIS
Epidemiology
The Nocardia sp. are aerobic, Gram-positive, filamentous, higher bacteria found worldwide in soil and decaying organic plant matter. They can be found in house dust, beach sand, garden soil, and swimming pools. They are able to cause disease in many organs, including the skin. Approximately 1000 cases of nocardiosis occur annually in the United States.6 Cutaneous disease comprises 5 percent to 22 percent of all cases. A higher incidence of primary cutaneous nocardiosis in Europe may be explained on the basis of more frequent isolation of N. brasiliensis in the environment. Patients have also been described in India and Argentina.4 Disease occurs most commonly in males.
Immunocompromised patients account for 50 percent of cases, mostly pulmonary,
systemic, and CNS infections. They are commonly seen in transplant patients, patients with acquired immunodeficiency syndrome (AIDS)4 or malignancy, or those receiving steroids. Primary cutaneous disease is most commonly seen in immunocompetent patients and has been reported rarely in children in United States, mostly in the south and southwestern part of the country.
Etiology and Pathogenesis
The Nocardia sp. of medical importance include N. asteroides, most commonly associated with lung and systemic disease, and N. brasiliensis, most commonly associated with skin infection. Other species include N. farcinica, N. otidiscaviarum, N. nova, N. pseudobrasilensis, N. transvalensis, and N. abscessus. It is only recently that many of this species have been completely separated, especially those of the N. asteroides group, including N. farcinica and N. nova. It is interesting to note that Nocardia sp. belong to a subgroup of bacteria called the aerobic nocardioform actinomycetes that also include Mycobacterium, Corynebacterium, Rhodococcus, and Gordona. All these microorganisms have mycolic acid as constituent of their cell wall, which explains the varying acid fastness on appropriate staining. The proposed etiologic agent for Whipple disease, Tropheryma whippelii, also belongs to this group.
The usual inflammatory response in infected tissue is neutrophilic, with branching, beading filamentous bacteria within abscesses. Sulfur granules are uncommon in primary cutaneous nocardiosis; they have been described in disseminated disease. They are more commonly seen when the clinical picture is that of mycetoma (see Actinomycetoma).
Clinical Findings
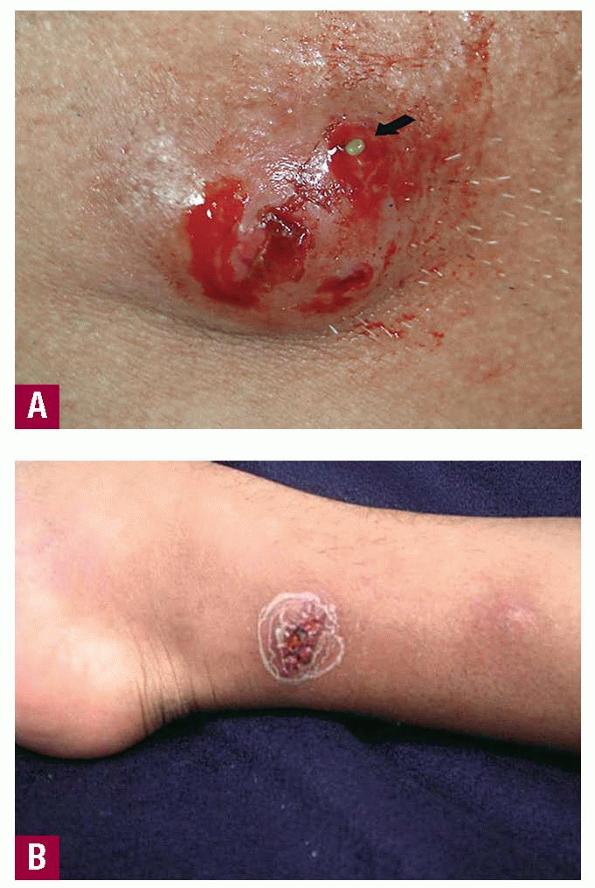
Cutaneous involvement by Nocardia can manifest either as cellulitis or more characteristically, as lymphocutaneous nodules in a sporotrichoid pattern. Disseminated disease can also present in the skin as a consequence of hematogenous spread. In most series, skin disease is second only to pulmonary involvement in frequency. Mycetoma due to Nocardia is discussed in Clinical Findings under Actinomycetoma.
Predisposing factors for primary cutaneous nocardiosis include soil or sand exposure while gardening or farming; or superficial injury from domestic shrubbery, outdoor falls, or accidents. The frequent history of thorn injury or gardening may suggest incorrectly a diagnosis of sporotrichosis. Cat scratches or insect bites may be also the portal of entry, especially in children.7
The most common cause of primary cutaneous nocardiosis is N. brasiliensis, but N. asteroides, N. otidiscaviarum, N. nova, and N. farcinica have also been implicated. Most patients are immunocompetent, but Nocardia cutaneous infection may also occur in the context of immunosuppression. A recent series of nocardial infection in AIDS patients showed skin lesions in 11 percent of cases, most commonly cutaneous abscesses and suppurative adenitis.
The disease has been also described in ulcerative bullous, linear/keloid, and nodulo-pustular forms that may evolve into the more specific sporotrichoid pattern . Patients may also present acutely with eccrine hidradenitis, or chronically with hyperkeratotic plaques. Cutaneous nocardiosis may begin suddenly, reactivate after months to years, or follow a chronic course for up to 10 years. A case of simultaneous infection in a husband and wife has also been described. Very rarely, pure cutaneous disease may lead to systemic illness. The cellulitic form most commonly affects the lower extremities, as compared to sporotrichoid form, in which the upper extremities are most commonly involved. Children frequently present with cellulitis, abscesses, and lymphadenitis affecting lower extremities and trunk; 20 percent of cases will have lesions at multiple sites.
Lymphocutaneous forms may account for 24 percent of all Nocardia cutaneous infections . The first case proven to be due to N. brasiliensis was described by Alarcon; the patient developed acute nodular suppurative lymphadenitis after injuring the finger with a rose thorn. Although the upper extremity is the most common location, disease of lower extremity and cervico-facial region have also been reported. A common history is appearance of a solitary papule or nodule on the upper limbs, 2 to 4 weeks after cutaneous inoculation. Then, proximal nodules develop along lymphatic drainage. The primary lesion is initially warm and tender, then becomes fluctuant and later ulcerates. Macroscopic grains may be seen, but draining sinuses are rare. Systemic symptoms are mild. Regional lymphadenitis is common but lymphangitis is unusual.
Sternal wound infections usually develop 1 month after thoracic surgery. The symptoms include erythema, clearto-purulent drainage, wound dehiscence, and/or fever. Diabetes mellitus seems to be the only identifiable risk factor. At least in one outbreak, the hands of an anesthesiologist were culture positive for N. farcinica. In another case of sternal osteomyelitis and mediastinal abscess, the patient's occupation (carrying wooden crates loaded with vegetables) may have been the source of infection, in the absence of chest surgery or trauma.
Pulmonary disease is the most common form of clinical infection, but, compared to primary cutaneous diseases, is often due to different species (N. asteroides predominates). The disease may take the form of an acute pneumonia or a chronic process with bronchopneumonia, abscesses, and development of cavities. Ten percent of pulmonary infections disseminates to the skin.
Bacteremia due to Nocardia is seen in patients with concomitant malignancy, and N. asteroides is the agent most commonly isolated. Cutaneous or subcutaneous nodules and abscesses occur in many patients, and the skin may be the portal of entry in some cases. Catheter-associated nocardemia is well documented.
Laboratory tests considered useful include direct examination of clinical specimens, culture, and biopsy. The importance
of direct microscopic examination for the presence of granules cannot be overemphasized. Organisms are detected as Gram-positive, branched filamentous “hyphae,” and branching at right angles is diagnostic. Acid-fast stains, including Fite-Faraco and the modified Kinyoun technique, show the filamentous bacteria. For isolation, cultures should be kept for up to 2 to 3 weeks. The microorganisms grow satisfactorily on most of the non-selective media used for isolation of bacteria, mycobacterium, and fungi. Because slow growth of Nocardia colonies over 2 days to 2 weeks on routine culture media allows bacterial overgrowth, isolation of this organism from soil and non-sterile sites may be difficult. Nocardia do not survive the digestive procedures used routinely in mycobacterial culture. Thayer-Martin and buffered charcoal-yeast extract agar may be used and pre-treatment of specimens with a low pH potassium chloride-hydrochloric acid solution for 4 minutes is required.
Patterns described on histology include monocytic infiltrates, fibrinopurulent exudates, granuloma formation, chronic granuloma formation, chronic nodular dermatitis, microabscess formation, and cocco-bacillary organisms; the presence of granules has been described in disseminated cases.
Differential Diagnosis
In cases of cellulitis, the differential diagnosis is extensive, including both infections and non-infectious etiologies. However, in the lymphocutaneous form, the differential diagnosis can be approached more systematically. The sporotrichoid pattern should be differentiated from the more acute ulcero-glandular syndrome, as is seen in tularemia and cat-scratch disease (Box 185-2).
Prognosis and Clinical Course
Primary cutaneous nocardiosis is usually subacute or chronic but has a good prognosis when treated appropriately. However, the disease has the potential to disseminate; sternal wound infections may be complicated with osteomyelitis. Systemic disease, especially sepsis, has a high mortality rate, 44 percent to 85 percent, if the patient is nocardemic.
Treatment
The treatment of Nocardia infection is appropriate antimicrobial therapy and surgical drainage and débridement. Factors to consider include site and severity of infection, the immune status of the host, potential for interactions and the species of Nocardia involved. Current standard for sensitivity testing is by the broth microdilution method.
Differential Diagnosis of Lymphocutaneous Nocardiosis
Most Likely
· Sporotrichosis
· Mycobacterium marinum infection
· Leishmaniasis
· Pyoderma due to Staphylococcus aureus
Consider
· Cryptococcosis
· Tuberculosis
· M. kansasii chelonae and M. fortuitum
· Cysticercosis
Rule Out
· Epithelioid sarcoma
· Metastatic disease
Sulfonamides, alone or in combination with trimethoprim (TMP), are the cornerstone of therapy for Nocardia infections, but are ineffective against N. otidiscaviarum. For primary cutaneous nocardiosis of mild to moderate intensity, sulfonamide (either sulfadiazine or sulfisoxazole) alone has been considered adequate therapy but other authors consider TMP-sulfamethoxazole (SMX) the treatment of choice, despite lack of controlled trials. This is based on synergistic activity of both drugs in vitro against Nocardia. The commercially available preparation has a fixed ratio of 1:5, and the dose recommended at the present time is 5 to 10 mg/kg TMP and 25 to 50 mg/kg SMX in two to four divided doses. For primary cutaneous nocardiosis, 5 mg/kg of TMP should be sufficient. Clinical improvement should be seen within 3 to 10 days, and 1 to 4 months of treatment should be curative for sporotrichoid nodules and cutaneous ulcers. Prolonged therapy is required for immunosuppressed patients. Minocycline 100 to 200 mg twice a day is considered the alternative treatment in cases of sulfonamide hypersensitivity or poor tolerance.
In more severe cases or disease involving other organs, a combination of sulfonamide with a second agent is recommended. The second-line drugs most recommended are amikacin, imipenem, and ceftriaxone. Alternative second-line drugs include amoxicillin-clavulanate and linezolid. Immunosuppression is a good indication for a two-drug regimen, including amikacin; 88 percent cure rate has been reported when this drug is used. Sternal infections due to N. asteroides have responded to oral ofloxacin therapy. N. farcinica has a high degree of resistance to various antibiotics, especially third-generation cephalosporin and imipenem, and combined therapy is highly recommended. Extended treatment for extra-cutaneous nocardiosis, with parenteral therapy followed by an oral regimen is necessary. Surgery is indicated in cases of abscesses (drainage) or extensive necrosis (débridement). Spontaneous resolution or good clinical response despite inappropriate therapy has been seen in children with Nocardia cellulitis or lymphadenitis.
Prevention
The low incidence of Nocardia infections in immunodeficient states does not justify prophylactic use of antibiotics. AIDS patients receiving TMP-SMX for Pneumocystis are already protected against Nocardia.