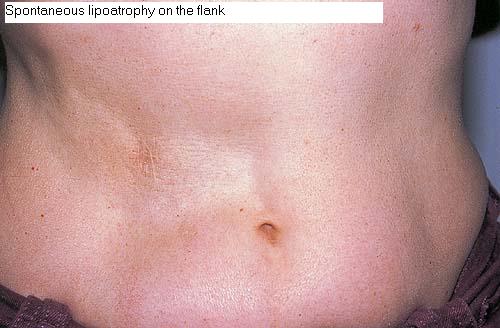
| Lipo atrophy = الضمور الشحمي |
|
|
Lipoatrophy
Often, lipoatrophy and lipodystrophy are used as synonymous terms, but from a pathogenic point of view, they are two different disorders that lead to loss of subcutaneous fat. Lipoatrophy refers specifically to a loss of subcutaneous fat due to a previous inflammatory process involving the subcutis. In contrast, lipodystrophy means an absence of subcutaneous fat with no evidence of inflammation. Lipodystrophy may be congenital or acquired, with total, partial, and localized lipodystrophy variants Several forms of localized lipoatrophy have been described according to their clinical appearance and location, namely annular lipoatrophy, abdominal lipoatrophy, semicircular lipoatrophy, and postinjection localized lipoatrophy. However, the most common localized lipoatrophy appears as a sequela of panniculitis, especially lupus panniculitis. Localized lipoatrophy may also appear at the sites of injection of different drugs, including corticosteroids, insulin, antibiotics, vasopressin, human growth hormone, and glatiramer acetate treatment for multiple sclerosis. Localized lipoatrophy secondary to pressure and compression by tight-fitting clothes has been also reported on the ankles, thighs, abdominal skin, and over the sacrum. In contrast, fully developed lesions of lipodystrophy show total absence of subcutaneous tissue with no evidence of inflammation, although some authors have postulated an early inflammatory stage From a histopathologic point of view, lipoatrophy is a residual process of several inflammatory conditions involving the subcutaneous fat lobules. In most cases, the histopathologic findings are those of lipophagic granulomas surrounding a small-sized fat lobule with perilobular fibrosis. In those cases of lipoatrophy secondary to subcutaneous injection of corticosteroids, two different histopathologic patterns have been described. Both patterns are characterized by the small size of the lobules and by the atrophy of the reduced number of adipocytes. The first pattern consists of faintly acidophilic small adipocytes that are retracted from the surrounding connective tissue of the septa. These changes are more prominent at the periphery of otherwise histologically normal fat lobules, suggesting that this is an early alteration of the lipoatrophic process. The general configuration of the fat lobule and the small size of the adipocytes resemble those of embryonic fat. Inflammatory cells are sparse, and blood vessels appear prominent, congested, and dilated. The second histopathologic pattern seen in lesions of lipoatrophy secondary to subcutaneous injections of corticosteroids is characterized by small, atrophic fat cells surrounded by a prominent vasculature. The small size of the fat lobule and adipocytes, the relative absence of inflammation, and the proliferation of small blood vessels give an angiomatous appearance to the fat lobule. In fully developed lesions of lipodystrophy, there is an absence of subcutaneous fat with deposition of new collagen, no evidence of inflammation, and the dermis and the fascia are in direct apposition. Recently, two histopathologic variants of lipodystrophy have been proposed. In the first type, there are prominent involutional changes in the fat lobule, with small adipocytes and intervening hyaline or myxoid connective tissue and proliferation of small blood vessels. The second type is the inflammatory type, because lymphocytes, foamy histiocytes, and plasma cells appear within the small fat lobules with normal-appearing adipocytes and vasculature. It is uncertain, however, whether or not these two patterns represent two different stages of a single process.
|