Linear Scleroderma.
Linear scleroderma is characterized by a band-like skin induration often with pigment changes, which may cross joint lines and sometimes leads to contractures . This form of LS occurs more commonly in children and on the extremities. The fibrotic process often may extend to the subcutaneous tissue, including fascia and muscle Joint contractures can be a significant cause of morbidity and deformities . In very young children, the process may affect bone growth and disrupt development of tissues. A “pansclerotic” process involving the entire extremity is seen in very severe cases. Pansclerotic morphea in children has been associated with an increased risk of cutaneous squamous cell carcinoma, particularly in ulcerated areas of affected skin.29,30
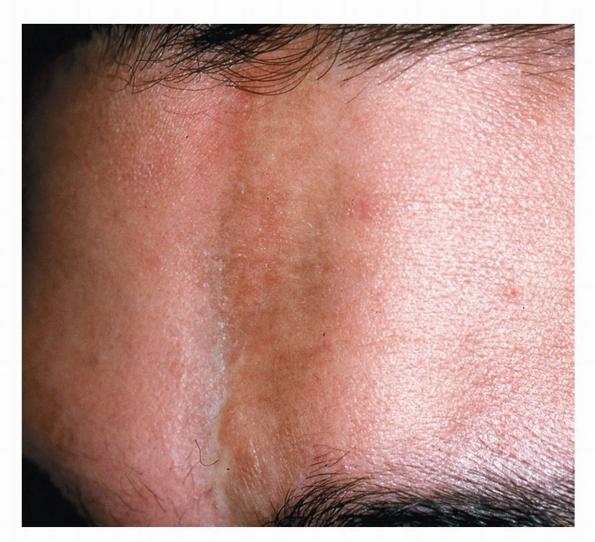
Linear scleroderma occurring on the face may present either as a purplishbrown streak or as a single white, atrophic band running vertically on the forehead, generally known as en coup de sabre . Progression to involve the scalp is common . If only the subcutaneous tissue, muscle, and, occasionally, bone are involved, this ipsilateral form
of LS is known as progressive facial hemiatrophy or Parry-Romberg syndrome . The extent of skin involvement and the development of facial hemiatrophy are not always directly correlated. Patients affected with facial lesions and Parry-Romberg syndrome fall within a spectrum of disease severity. Mildly affected patients may have only a single linear atrophic band. Severely affected patients may have facial hemiatrophy with loss of subcutaneous tissue, muscle, and bone as well as atrophy of the tongue and salivary glands on the same side. Severely affected patients may also have central nervous system involvement of the meninges and brain with the potential for seizures, headaches, and vision changes.
Eosinophilic Fasciitis.
EF, or Shulman syndrome, is a related disorder that presents with the rapid onset of symmetric areas of edema on the extremities . The condition progresses over several weeks to cutaneous induration and contractures, with features similar to those of subcutaneous forms of LS. Up to 30 percent to 40 percent of patients with EF have lesions indistinguishable from LS.
Atrophoderma of Pasini and Pierini.Atrophoderma of Pasini and Pierini is present in many patients with LS and presents with oval blue to dark brown hyperpigmented atrophic and slightly depressed areas. There is generally no induration or violaceous border in these lesions, in contrast to plaque-type morphea. The borders of the atrophoderma lesions have a “cliff-drop” appearance . Some consider atrophoderma to be an aborted, superficial form of LS