ACRODERMATITIS
CHRONICA
ATROPHICANS
Clinical Features.
Observed mainly in elderly patients in Europe, ACA has an insidious onset and appears to have predilection for females.66 Rare cases of ACA have been reported in children.67 The time interval from the spirochete inoculation
to the onset of symptoms of ACA is extremely difficult to evaluate. Most patients do not recall the specific tick bite that initiated the disease.That the spirochete can survive for decades is favored by reports indicating transmission of the disease from ACA patients even after 20 years.
Cutaneous Manifestations of Lyme Disease
|
|
|
|
ONSET
|
DIAGNOSIS/DIFFERENTIAL DIAGNOSIS
|
|
COMMON MANIFESTATIONS
|
|
|
|
Erythema migrans
|
Weeks to months (early)
|
Arthropod bite, erythema multiforme granuloma annulare, urticaria, erysipelas, brown recluse spider bite, fixed drug eruption
|
|
Acrodermatitis chronica atrophicans
|
Months to years (late)
|
Venous insufficiency, lichen sclerosus, scleroderma, physiologic age-related atrophy, corticosteroid-induced atrophy
|
|
UNCOMMON MANIFESTATIONS
|
|
|
|
Cutaneous scleroborrelioses
|
Months to years (late)
|
|
|
|
Morphea
|
|
Primary morphea
|
|
|
Lichen sclerosus et atrophicus
|
|
Primary lichen sclerosus et atrophicus
|
|
|
Periarticular fibrous nodules
|
|
Rheumatoid nodule, gouty tophi
|
|
|
Progressive facial hemiatrophy
|
|
Primary progressive facial hemiatrophy/Parry-Romberg syndrome
|
|
|
Eosinophilic fasciitis
|
|
Primary eosinophilic fasciitis/Shulman syndrome
|
|
Cutaneous atrophoborrelioses
|
Months to years (late)
|
|
|
|
Anetoderma
|
|
Primary anetoderma
|
|
Cutaneous lymphoborrelioses
|
Months to years (late)
|
|
|
|
B-cell dominant (including B-cell lymphoma)
|
|
Arthropod bite reaction, response to vaccination, granulomas, neoplasm
|
|
|
T-cell dominant
|
|
Pityriasis lichenoides, polymorphous light eruption
|
|
Other cutaneous lesions
|
Weeks to months to years (early or late)
|
|
|
|
Panniculitis
|
Erythema nodosum
|
|
|
Granuloma annulare
|
|
Insect bite reaction
|
|
|
Erythema multiforme
|
|
Drug eruption
|
|
|
Syphilis-like papulo-squamous eruption
|
|
Secondary syphilis
|
|
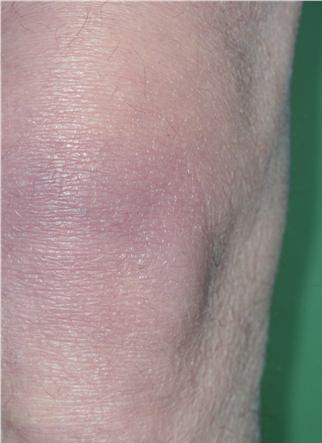
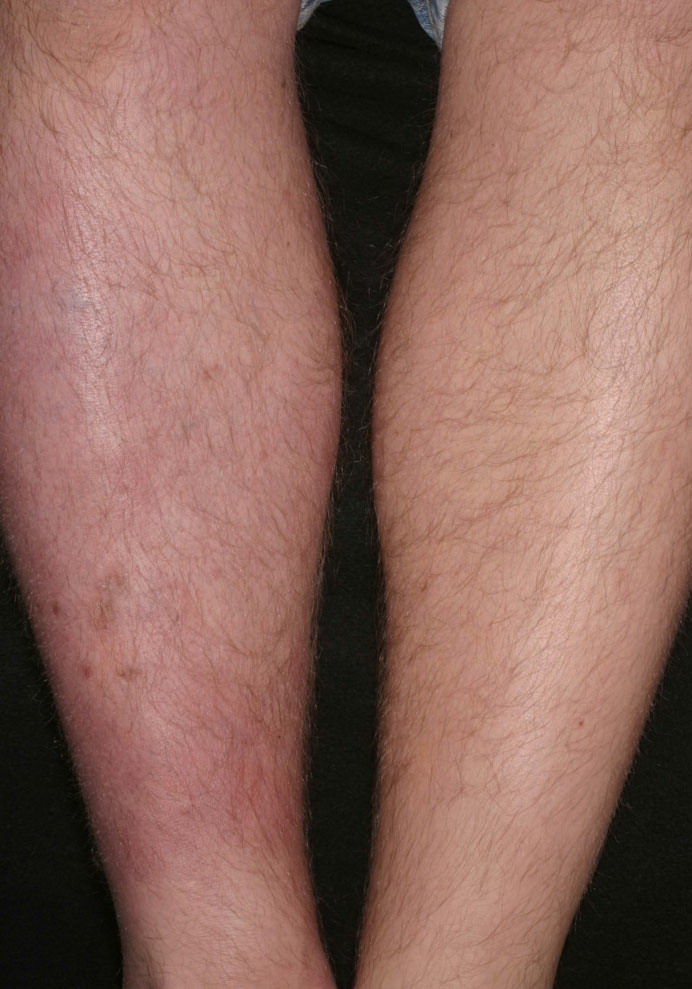
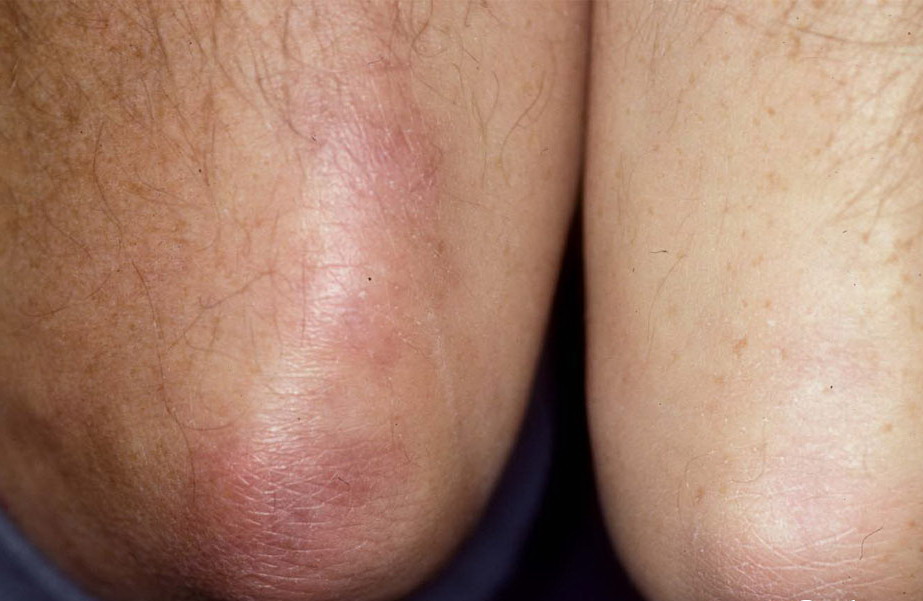
An inflammatory phase characterizes the early clinical stages of this biphasic disease. The inflammatory phase presents as a bluish-red discoloration on the extensor aspect of fingers, hands, joints, and lower extremities . Joints usually involved include the elbows and knees. Infiltrated purple bands of varying widths may be observed adjacent to involved joint(s). Associated findings include a cushion-like (“doughy”) swelling of the dorsum of the hands and feet (see eFig. 187-3.2 in on-line edition).69 The extremities are most commonly involved, although extensive lesions on the trunk have also been documented. Lesions typically extend from the distal to the proximal portion of the extremity involved. Although the erythema and swelling initially vary in intensity (“waxes and wanes”), swelling of the posterior aspect of the lower extremities is believed by some to be particularly indicative of Lyme disease.
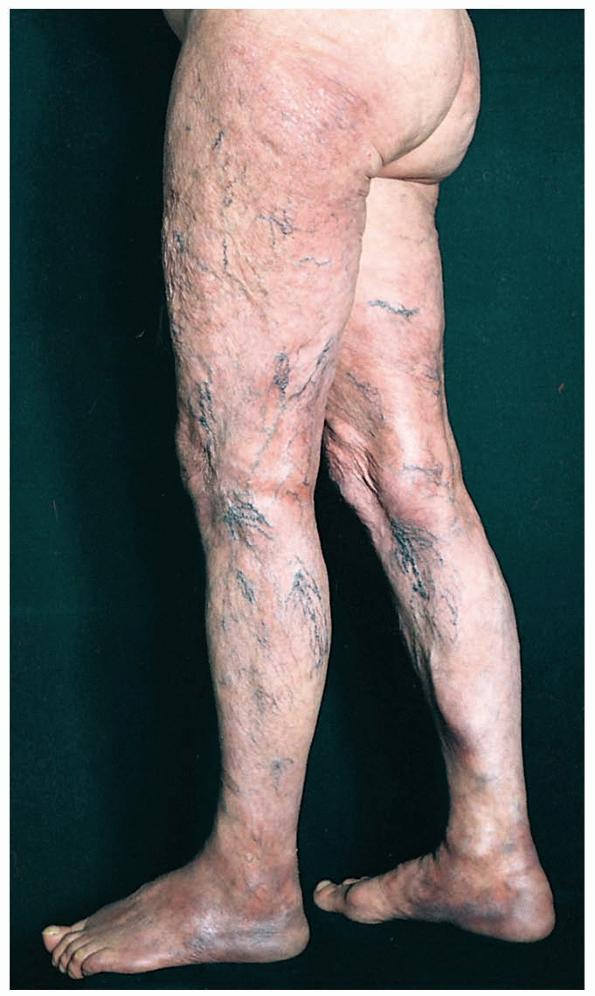
Cutaneous atrophy characteristic of the later clinical stage is not an obligatory sequel to the inflammatory phase of ACA. Rarely, coexistence of both kinds of lesions at different sites in the same patient has been documented. The atrophic phase is characterized by lesions with a “cigarette paper-like” appearance and a prominence of superficial veins (.
Extracutaneous Features.
Central and peripheral nervous system involvement has also been documented in approximately 45 percent of patients with ACA. Thirty percent to 45 percent of patients suffer from a polyneuropathy, often most pronounced in the limb with cutaneous involvement. Chronic joint and bone involvement, attributed to persistence of spirochetes in cutaneous lesions, is most often seen in patients with long-standing ACA or an untreated lesion of EM/ACA and is typically restricted to the extremity involved. The characteristic symptom, exhibited in approximately one-third of patients in one study, was a swollen or painful foot and heel. Other symptoms include subluxation of small joints, bursitis, arthritis, and cortical thickening of bone. Solitary or multiple fibrotic lesions near joints, particularly in the olecranon area, may develop in some patients.
Histologic Features.
All three species of B. burgdorferi that infect humans have been found in ACA lesions. Histopathologic features of biopsied lesions vary with the clinical phase of ACA. In inflammatory lesions, three layers are typically described: an atrophic epidermis, a zone of uninvolved papillary dermis, and a layer of inflammatory cells composed of lymphocytes
and plasma cells. The presence of plasma cells in the infiltrate is documented mainly from studies from Europe, as American reports indicate that few or no plasma cells are found. The infiltrate may be deep with extension into the subcutis. Occasionally, interface dermatitis has been reported. Unusual findings include the presence of vacuoles, either singly or in groups, at different levels of the dermis.73 Although some believe these represent mature adipocytes, others believe them to be an expression of lymphedema, given that they are mainly observed from biopsies of markedly edematous sites. In favor of the latter hypothesis is the absence of such vacuoles from the same site post-treatment.
Phenotypic studies indicate the lymphocytes in the infiltrate are mainly of the CD4 phenotype, favoring the concept that ACA is a T cell-mediated immune response. Further in support of this theory is the expression of adhesion molecules, such as intracellular adhesion molecule-1, on endothelial cells, lymphocytes, and basal keratinocytes in the inflammatory infiltrate. Chronicity of the lesions may be partially explained by down-regulation of major histocompatibility complex class II molecules on Langerhans cells.
Diagnosis and Differential Diagnosis.
Lesions of ACA are notoriously overlooked or misinterpreted. In those with a relevant clinical history, the onset appears to be related to an untreated lesion of EM and/or neurologic manifestations. In one study, a history of EM months to years earlier on the same side was found in approximately 18 percent of patients.
Detection of the spirochete substantiates the infective etiology, further supported by positive serologic findings. The latter are of great utility in the diagnosis of ACA. Antibodies to B. burgdorferi can be detected in almost all (100 percent) of patients with ACA even years after treatment.